 PDF
PDF  Views
Views  Share
Share


Weekly versus Tri-weekly Cisplatin Concurrent with Radiotherapy in the Treatment of Locally Advanced Carcinoma Cervix: A Prospective Study
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2018; 39(04): 467-472
DOI: DOI: 10.4103/ijmpo.ijmpo_89_17
Abstract
Context: Different schedules of concurrent chemotherapy with definitive radiotherapy in locally advanced carcinoma cervix. Aims: The aim is to evaluate toxicity, compliance, and response of weekly versus tri-weekly cisplatin given concurrently with radiotherapy in locally advanced squamous cell carcinoma cervix. Subjects and Methods: One hundred and ten newly diagnosed histopathologically confirmed squamous cell carcinoma cervix patients with International Federation of Gynecologists and Oncologists stage IIB to IVA were randomly distributed among study group receiving 75 mg/m2 of cisplatin every 3 weeks for three cycles and control group receiving 40 mg/m2 of weekly cisplatin for six cycles. Results: Patients in both the arms tolerated treatment well. At the time of completion of chemoradiotherapy, 83.63% of patients of the study group and 80% of the control group had a complete response whereas 16.37% of study and 20% of the control group had a partial response, both statistically insignificant (P > 0.05). Compliance was similar in both the groups. The average time to complete radiotherapy was 54.63 days in the study group and 51.34 days in the control group. In the study group, 87.27% of patients completed all cycles of tri-weekly chemotherapy, whereas, in control group, 80% completed all 6 cycles of weekly chemotherapy. The difference was not statistically significant (P = 0.30). Toxicity in terms of vomiting, grade 3–4 leukopenia and neutropenia were more in the study group which was statistically significant (P < 0 class="i" xss=removed>P = 0.04, and P = 0.03, respectively). Conclusions: Although the 3-weekly cisplatin schedule has longer intervals and sounds convenient, the weekly cisplatin regime shows lower hematologic toxicity with similar disease response and compliance.
Keywords
Cervical cancer - concurrent chemoradiation - Cisplatin - external-beam radiotherapy - International Federation of Gynecology and Obstetrics - high dose rate intracavitary brachytherapyPublication History
Article published online:
17 June 2021
© 2018. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Context: Different schedules of concurrent chemotherapy with definitive radiotherapy in locally advanced carcinoma cervix. Aims: The aim is to evaluate toxicity, compliance, and response of weekly versus tri-weekly cisplatin given concurrently with radiotherapy in locally advanced squamous cell carcinoma cervix. Subjects and Methods: One hundred and ten newly diagnosed histopathologically confirmed squamous cell carcinoma cervix patients with International Federation of Gynecologists and Oncologists stage IIB to IVA were randomly distributed among study group receiving 75 mg/m2 of cisplatin every 3 weeks for three cycles and control group receiving 40 mg/m2 of weekly cisplatin for six cycles. Results: Patients in both the arms tolerated treatment well. At the time of completion of chemoradiotherapy, 83.63% of patients of the study group and 80% of the control group had a complete response whereas 16.37% of study and 20% of the control group had a partial response, both statistically insignificant (P > 0.05). Compliance was similar in both the groups. The average time to complete radiotherapy was 54.63 days in the study group and 51.34 days in the control group. In the study group, 87.27% of patients completed all cycles of tri-weekly chemotherapy, whereas, in control group, 80%-completed all 6 cycles of weekly chemotherapy. The difference was not statistically significant (P = 0.30). Toxicity in terms of vomiting, grade 3–4 leukopenia and neutropenia were more in the study group which was statistically significant (P < 0 class="i" xss=removed>P = 0.04, and P = 0.03, respectively). Conclusions: Although the 3-weekly cisplatin schedule has longer intervals and sounds convenient, the weekly cisplatin regime shows lower hematologic toxicity with similar disease response and compliance.
Keywords
Cervical cancer - concurrent chemoradiation - Cisplatin - external-beam radiotherapy - International Federation of Gynecology and Obstetrics - high dose rate intracavitary brachytherapyIntroduction
Cervical cancer is the second most common cancer diagnosed in women in India.[1] About 122,844 new cervical cancer cases are diagnosed annually in India.[2] At our center, carcinoma cervix is the most common cancer among females. Patients usually present to us with International federation of Gynecology and Obstetrics (FIGO) stage IIB, III and IV; in which Concurrent Chemo-Radiotherapy (CCRT) plays a major role in the management.[3] [4]
Subjects and Methods
The present prospective study was carried out at Sawai Man Singh Medical College and attached group of Hospitals, Jaipur, Rajasthan from January 2014 to June 2015 with a median follow up of 33 months. 110 histopathologically confirmed newly diagnosed cases of squamous cell carcinoma of cervix FIGO stage IIB to IVA with ECOG performance status 0–2 were randomised into study and control groups, with 55 patients in both groups. All patients were younger than 70 but older than 18 years with hemoglobin ≤9 g%, absolute neutrophil count >1500/uL, platelet count >1,00,000/uL, serum creatinine level <1>
Chemotherapy
All patients who were enrolled in the study group were planned to receive injection cisplatin with dose of 75 mg/m2 intravenously on day 1, 22, and 43 of radiotherapy, for a total of three courses. Those who were enrolled in the control arm were planned to receive injection cisplatin with dose of 40 mg/m2 intravenously on day 1, 8, 15, 22, 29, and 36 of radiotherapy, for a total of six courses.
Radiotherapy
Combined external-beam radiotherapy (EBRT) and high dose rate intracavitary brachytherapy (HDR ICBT) was used for the treatment of patients. The primary tumor and regional lymphatics were treated with 45–50.4 Gy in conventional fractionation at 1.8 Gy per fraction over Seimens Oncor Expression Linear Accelerator using three-dimensional conformal radiotherapy technique with 15 MV beam energy. The first HDR ICBT was performed toward the latter part of EBRT when sufficient tumor regression was noted to permit satisfactory applicator geometry. This was usually after the 3rd week of EBRT and additional EBRT was delivered with a central shield. On the day of ICBT, neither EBRT nor chemotherapy was prescribed. The recommended total point A dose combining EBRT with ICBT was 80 Gy for small volume cervical tumors and 85–90 Gy for large volume tumors. To avoid the negative impact of treatment prolongation, the overall treatment time was intended to be kept <8 href="https://www.thieme-connect.com/products/ejournals/html/10.4103/ijmpo.ijmpo_89_17#JR_5" xss=removed>5] [6]
Evaluation of patients
All patients were clinically examined weekly during the treatment for any complaints. Hemogram and biochemical investigations were performed and noted before giving chemotherapy. The clinical appearance of the primary tumor at the initiation of treatment was noted. The regression of primary tumor during the treatment was assessed and noted biweekly. Any delay causing treatment interruption was also noted and necessary gap correction for radiotherapy was done. Chemotherapy was withheld during radiotherapy interruptions, but radiotherapy was continued in spite of chemotherapy being discontinued due to hematological toxicities. At the completion of treatment and subsequent follow up, the disease response was assessed. The results of study group were analyzed and compared with control group in terms of compliance, toxicities, and tumor response. Response was assessed as per the WHO Criteria. Acute toxicities were assessed as per the Radiation Therapy Oncology Group (RTOG) Acute Radiation Morbidity Scoring criteria. Chemotherapy induced toxicities such as nausea, vomiting, renal and hematological toxicities were assessed as per the CommonTerminology Criteria for Adverse Events (v4.03), National Cancer Institute (USA). Patients were evaluated every month on follow up with detailed clinical examination to assess local disease response and to note any bladder/bowel symptom. Hematological tests and imaging studies were done wherever indicated.
Statistical analysis
This was an open-label, randomized trial with 1:1 allocation. The randomized assignment was done using a chit in box method with replacement. The categorical clinical characteristics between the two treatments were compared using Chi-square (χ2) test. Data were analyzed using Statistical Package for Social Sciences (SPSS) software trial version 20.0 (IBM Corp., Armonk, New York, USA).
Results
In the present study, the patient and tumor characteristics were identical in the two groups [Table 1]. In both the groups, patients were in the age group of 30–70 and majority of them were in their 4th and 5th decade of life. Mean age of presentation was 49.36 and 49.43 years for study and control group, respectively. More than two-third of the patients belonged to the rural background in both the groups. All the patients included in the study were having ECOG performance status score up to 2. The hemoglobin of all patients included in the study was equal or above 9.0 g%, mean hemoglobin at presentation was 10.56 g%-and 10.60 g% for study and control group, respectively. Only histopathologically proven squamous cell carcinoma patients were included in this study. The distribution of patients according to the histological differentiation of primary tumor revealed moderately differentiation as the most common pattern of differentiation. Among the study group, 78.2%-and in the control group, 81.8%-had moderately differentiated tumor. The most common stage of presentation was FIGO stage IIB with 54.5%-in the study group and 50.9%-in control group.
|
Study group, n (%) |
Control group, n (%) |
P value |
|
|---|---|---|---|
|
ECOG – Eastern cooperative oncology group; FIGO – International federation of gynecology and obstetrics |
|||
|
Age (years) |
|||
|
≤40 |
9 |
13 |
0.15 |
|
41-50 |
25 |
18 |
|
|
51-60 |
16 |
12 |
|
|
61-70 |
5 |
12 |
|
|
Geographic distribution |
|||
|
Rural |
38 (69) |
37 (67.3) |
0.84 |
|
Urban |
17 (31) |
18 (32.7) |
|
|
ECOG performance status |
|||
|
0 |
0 |
0 |
0.54 |
|
1 |
50 (91) |
48 (87.3) |
|
|
2 |
5 (9) |
7 (12.7) |
|
|
FIGO stage |
|||
|
IIB |
30 (54.5) |
28 (50.9) |
0.70 |
|
IIIA |
2 (3.6) |
1 (1.9) |
|
|
IIIB |
22 (40) |
23 (41.8) |
|
|
IVA |
1 (1.9) |
3 (5.4) |
|
|
Differentiation of squamous cell carcinoma |
|||
|
Well differentiated |
10 (18.2) |
7 (12.7) |
0.68 |
|
Moderately differentiated |
43 (78.2) |
45 (81.8) |
|
|
Poorly differentiated |
2 (3.6) |
3 (5.5) |
|
|
Duration of radiotherapy (weeks) |
|||
|
≤8 |
48 |
52 |
0.18 |
|
>8 |
7 |
3 |
|
|
Toxicity |
Study group |
Control group |
Statistics |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Grade 0 |
Grade 1 |
Grade 2 |
Grade 3 |
Grade 4 |
Grade 0 |
Grade 1 |
Grade 2 |
Grade 3 |
Grade 4 |
P Value |
|
|
TLC – Total leukocyte counts; ANC – Absolute neutrophil counts |
|||||||||||
|
Acute skin reaction |
0 |
10 |
34 |
11 |
0 |
2 |
20 |
26 |
7 |
0 |
0.06 |
|
Nausea during treatment |
0 |
17 |
31 |
7 |
0 |
0 |
23 |
25 |
7 |
0 |
0.46 |
|
Vomitting during treatment |
0 |
5 |
27 |
23 |
0 |
7 |
23 |
21 |
4 |
0 |
<0> |
|
Acute diarrhea |
12 |
31 |
12 |
0 |
0 |
16 |
23 |
12 |
4 |
0 |
0.12 |
|
Heamoglobin |
0 |
21 |
34 |
0 |
0 |
0 |
20 |
35 |
0 |
0 |
0.84 |
|
TLC |
29 |
14 |
10 |
2 |
0 |
37 |
16 |
2 |
0 |
0 |
0.04 |
|
ANC |
36 |
8 |
9 |
2 |
0 |
48 |
5 |
2 |
0 |
0 |
0.03 |
|
Nephrotoxicity |
45 |
10 |
0 |
0 |
0 |
48 |
7 |
0 |
0 |
0 |
0.43 |
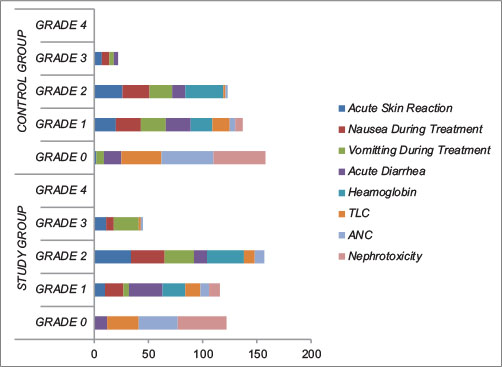
| Figure 1:Worst Acute Toxicity During Treatment
As far as hematological toxicities are concerned, in the study group 21 (38.2%) had grade 1 and 34 (61.8%) had grade 2 anemia, whereas in control group, 20 (36.4%) had grade 1 and 35 (63.6%) had grade 2 anemia (P = 0.84). For total leukocyte counts, study group had more grade 2 (10 [18.2%]) and grade 3 toxicity (2 [3.6%]) compared to control group having only 2 (3.6%) grade 2 toxicity. 14 (25.5%) and 16 (29.09%) had grade 1 toxicity in study and control group, respectively. This difference is statistically significant, showing more toxicity in the study group compared to control group, P = 0.04. Similar to total leucocyte count, absolute neutrophil count showed the same pattern of toxicity profile. 36 (65.5%) and 48 (87.3%) had no toxicity, 8 (14.5%) and 5 (9.09%) had grade 1, 9 (16.4%) and 2 (3.6%) had grade 2 and 2 (3.6%) and none (0%) had grade 3 toxicity in the study and control group, respectively. This difference was statistically significant, more in the study group compared to control group (P = 0.03). No nephrotoxicity was found in 45 (81.8%) in the study group and 48 (87.3%) in the control group, whereas 10 (18.2%) and 7 (12.7%) were found to have grade 1 toxicity in the study and control group, respectively (P = 0.43). The audiometry report of all the patients was comparable to their pretreatment and post treatment reports, i.e., there was no increased hearing loss or ototoxicity found among all the patients in both study and control group.
Compliance of the treatment was defined in terms of completeness of chemotherapy and radiotherapy within the prescribed time limits. The American Brachytherapy Society recommends keeping the total treatment duration to <8 href="https://www.thieme-connect.com/products/ejournals/html/10.4103/ijmpo.ijmpo_89_17#JR_7" xss=removed>7] In the study group, the average time of completion of radiotherapy was 54.63 days, (range = 48–81 days), 48 (87.27%) patients completed their radiotherapy within 56 days (8 weeks) of starting treatment. Whereas in the control group, the average time was 51.34 days, (range = 48–60 days), 52 (94.54%) patients completed within the prescribed time of 56 days (8 weeks). This difference did not reach statistical significance (P = 0.18).
Treatment response of disease of patients was done using the WHO criteria while on treatment and subsequent follow up. At the end of treatment, 46 (83.63%) of study group and 44 (80%) of control group had complete response (CR), 9 (16.37%) patients of study group and 11 (20%) patients of control group had partial response (PR) (P = 0.62). At 6 months after completion of CCRT, both the study and control group had 50 (90.9%) CR and 5 (9.1%) PR rates (P = 1). At last follow up, the disease-free survival was same for both the study and control group [Table 3].
|
Treatment response |
Study group (n) |
Control group (n) |
Statistics |
||||||
|---|---|---|---|---|---|---|---|---|---|
|
Complete response |
Partial response |
No change |
Progressive disease |
Complete response |
Partial response |
No change |
Progressive disease |
P value |
|
|
End of treatment |
46 |
9 |
0 |
0 |
44 |
11 |
0 |
0 |
0.63 |
|
6 month follow up |
50 |
5 |
0 |
0 |
50 |
5 |
0 |
0 |
1.00 |
| Figure 1:Worst Acute Toxicity During Treatment
References
- National cancer registry programme. Indian council of medical research, three year report of population based cancer registries 2012-2014, Incidence, Distribution, Trends in Incidence Rates and Projections of Burden of Cancer. Bengluru:India 2016; 2: 9-26 Available from: http://www.ncrpindia.org/ALL_NCRP_REPORTS/PBCR_REPORT_2012_2014/ALL_CONTENT/PDF_Printed_Version/Chapter2_Printed.pdf. [Last accessed on 2017 Jul 15].
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C. et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer; 2013. Available from: http://www.globocan.iarc.fr/factsheet.asp. [Last accessed on 2017 Oct 17].
- Viswanathan AN. Uterine Cervix. In: Halperin EC, Wazer DE, Perez CA, Brady LW. editor Principles and practice of radiation oncology. 6th ed. Philadelphia: Lippincott Williams and Wilkins; 2013: 1355-9
- Rose PG, Bundy BN, Watkins EB, Thigpen JT, Deppe G, Maiman MA. et al. Concurrent cisplatin-based radiotherapy and chemotherapy for locally advanced cervical cancer. N Engl J Med 1999; 340: 1144-53
- Perez CA, Grigsby PW, Castro-Vita H, Lockett MA. Carcinoma of the uterine cervix. I. Impact of prolongation of overall treatment time and timing of brachytherapy on outcome of radiation therapy. Int J Radiat Oncol Biol Phys 1995; 32: 1275-88
- Chen SW, Liang JA, Yang SN, Ko HL, Lin FJ. The adverse effect of treatment prolongation in cervical cancer by high-dose-rate intracavitary brachytherapy. Radiother Oncol 2003; 67: 69-76
- Nag S, Erickson B, Thomadsen B, Orton C, Demanes JD, Petereit D. The American Brachytherapy Society recommendations for high-dose-rate brachytherapy for carcinoma of the cervix. Int J Radiat Oncol Biol Phys 2000; 48: 201-11
- Keys HM, Bundy BN, Stehman FB, Muderspach LI, Chafe WE, Suggs 3rd CL. et al. Cisplatin, radiation, and adjuvant hysterectomy compared with radiation and adjuvant hysterectomy for bulky stage IB cervical carcinoma. N Engl J Med 1999; 340: 1154-61
- Morris M, Eifel PJ, Lu J, Grigsby PW, Levenback C, Stevens RE. et al. Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. N Engl J Med 1999; 340: 1137-43
- Whitney CW, Sause W, Bundy BN, Malfetano JH, Hannigan EV, Fowler Jr. WC. et al. Randomized comparison of fluorouracil plus cisplatin versus hydroxyurea as an adjunct to radiation therapy in stage IIB-IVA carcinoma of the cervix with negative para-aortic lymph nodes: A Gynecologic Oncology Group and Southwest Oncology Group study. J Clin Oncol 1999; 17: 1339-48
- Green JA, Kirwan JM, Tierney JF, Symonds P, Fresco L, Collingwood M. et al. Survival and recurrence after concomitant chemotherapy and radiotherapy for cancer of the uterine cervix: A systematic review and meta-analysis. Lancet 2001; 358: 781-6
- Green J, Kirwan J, Tierney J, Vale C, Symonds P, Fresco L. et al. Concomitant chemotherapy and radiation therapy for cancer of the uterine cervix. Cochrane Database Syst Rev 2005; 3: CD002225
- Serkies K, Jassem J. Concurrent weekly cisplatin and radiotherapy in routine management of cervical cancer: A report on patient compliance and acute toxicity. Int J Radiat Oncol Biol Phys 2004; 60: 814-21
- Kato S, Ohno T, Thephamongkhol K, Chansilpa Y, Yuxing Y, Devi CR. et al. Multi-institutional phase II clinical study of concurrent chemoradiotherapy for locally advanced cervical cancer in East and Southeast Asia. Int J Radiat Oncol Biol Phys 2010; 77: 751-7
- Ryu SY, Lee WM, Kim K, Park SI, Kim BJ, Kim MH. et al. Randomized clinical trial of weekly vs. triweekly cisplatin-based chemotherapy concurrent with radiotherapy in the treatment of locally advanced cervical cancer. Int J Radiat Oncol Biol Phys 2011; 81: e577-81
- Chumworathayi B, Suprasert P, Charoenkwan K, Srisomboon J, Phongnarisorn C, Siriaree S. et al. Weekly versus three-weekly cisplatin as an adjunct to radiation therapy in high-risk stage I-IIA cervical cancer after surgery: A randomized comparison of treatment compliance. J Med Assoc Thai 2005; 88: 1483-92
- Ikushima H, Osaki K, Furutani S, Yamashita K, Kawanaka T, Kishida Y. et al. Chemoradiation therapy for cervical cancer: Toxicity of concurrent weekly cisplatin. Radiat Med 2006; 24: 115-21
- Kim YS, Shin SS, Nam JH, Kim YT, Kim YM, Kim JH. et al. Prospective randomized comparison of monthly fluorouracil and cisplatin versus weekly cisplatin concurrent with pelvic radiotherapy and high-dose rate brachytherapy for locally advanced cervical cancer. Gynecol Oncol 2008; 108: 195-200
- Toita T, Moromizato H, Ogawa K, Kakinohana Y, Maehama T, Kanazawa K. et al. Concurrent chemoradiotherapy using high-dose-rate intracavitary brachytherapy for uterine cervical cancer. Gynecol Oncol 2005; 96: 665-70