 PDF
PDF  Views
Views  Share
Share


Unusual coexistence of a renal anomaly and germ cell tumor: An embryonal happenstance?
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2012; 33(03): 179-181
DOI: DOI: 10.4103/0971-5851.103150
Abstract
The germ cell lines and kidney develop in close proximity in a similar embronic period. The extragonadal germ cell tumors and horseshoe kidney both are the result of abnormal migration of two germ line cells. Apart from origin, the combined incidence of mediastinal germ cell tumor with renal anomaly is a therapeutic challenge. This case review is an effort to address the various issues ranging from delima in origin to management and follow-up.
Publication History
Article published online:
02 August 2021
© 2012. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
The germ cell lines and kidney develop in close proximity in a similar embronic period. The extragonadal germ cell tumors and horseshoe kidney both are the result of abnormal migration of two germ line cells. Apart from origin, the combined incidence of mediastinal germ cell tumor with renal anomaly is a therapeutic challenge. This case review is an effort to address the various issues ranging from delima in origin to management and follow-up.
INTRODUCTION
Extra-gonadal germ cell tumors (EGGCT) most commonly present in the midline of the body (retroperitoneum, mediastinun, pineal region).[1] EGGCT non-seminomatous tumors have been associated with Klinefelter syndrome (20%)[2] but rarely with other congenital anomalies. We describe an unusual case of a young adult who presented with EGGCT and a horseshoe kidney (HSK) and was successfully treated with chemotherapy, surgery and repeat surgery for a recurrent mass. We postulate an intraembryonic event occurring at the same time during organogenesis as the cause for this unique association.
CASE REPORT
A 30-year-old gentleman presented to us with a 1-month history of left-sided chest pain. The positron emission tomography (PET)-computed tomography (CT) scan revealed a 13.3 cm × 14 cm mass in the left upper mediastinum (SUV Max 21.4) and an incidental HSK [Figure [Figure1a1a and andb].b]. The testes were normal. A CT-guided biopsy of the mass revealed germ cell (Yolk sac) tumor, positive for CK, AFP and negative for C-kit, TTF1, CK7 and CD30. The serum alpha fetoprotein (AFP), beta human chorionic gonadotrophic hormone (β HCG) and lactate dehydrogenase (LDH) values were 16,093 ng/mL, < 1.2 Miu/mL and 1013 U/L, respectively. The patient received chemotherapy with Paclitaxel (250 mg/m2; Day 1), Ifosphamide (1.2 gm/m2, Days 2-5) and Cisplatin (40 mg/ m2, Days 2–5) three weekly for four cycles (TIP).
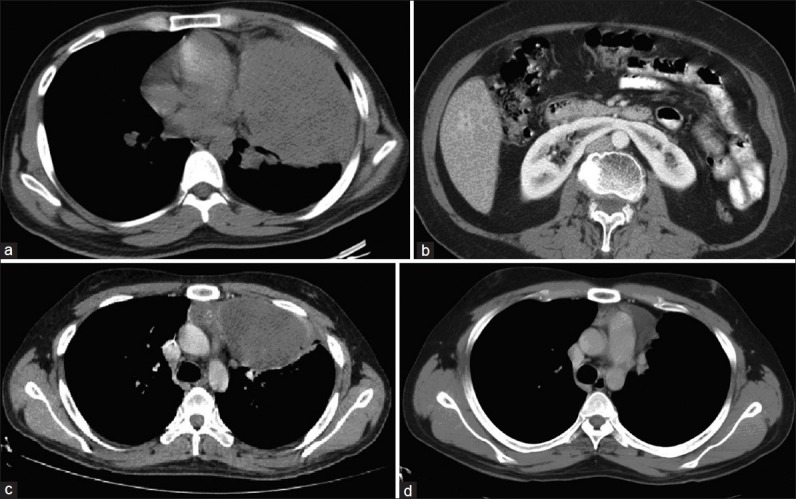
| Fig. 1 (a) Mediastinal mass at diagnosis, (b) Horseshoe kidney, (c) Mediastinal residual mass post chemotherapy, (d) Mediastinal recurrence post surgery
The post-chemotherapy CT scan of the chest showed a residual mediastinal mass [Figure 1c]. There was a decreasing trend in serum markers (AFP 39.8 ng/mL, β HCG < 1.2 Miu/mL and LDH 250 U/L). The mass was subsequently excised and histopathology revealed a necrotic mass with no residual viable tumor. After 5 months, the patient presented with recurrent cough and raised serum LDH levels. The PET-CT scan showed a 3.2 cm × 5.2 cm recurrent mass in the anterior mediastinum (Max SUV 10.1) [Figure 1d]. The re-excision of the tumor was done and histopathology showed a mature teratoma. The patient is currently on regular follow-up and is asymptomatic, disease free radiologically and biochemically.
DISCUSSION
Nearly 20% of all EGGCT non-seminomatous tumors have Klinefelter's syndrome.[2] There is no documented literature on any other association of gonadal or EGGCT with congenital abnormalities. The HSK is the most common type of renal fusion anomaly and can be related to teratogenic events affecting the urinary system (Wilms tumor and carcinoid tumors).[2] Kidney is one of the least common locations for EGGCT teratomas, with only one case report of a child with HSK and intrarenal teratoma.[3]
The development of the genital apparatus accompanies that of the urinary system.[4] The intermediate mesoblast consists of two components, genital ridge forming gonads and nephrogenic cord forming mesonephros of the urinary apparatus. The genital ridge with primordial germ cells (PGC) extends from the upper thoracic region to the level of the cloaca, but true gonads develop through the middle area only and descends from the lumbar area (ventromedial to the mesonephros) to the future scrotum (9–12th weeks). The pathologic PGC ectopic localization during migration causes EGGCT. The metanephros from nephrogenic cord in the sacral region ascends passively due to differential growth of the lumbar and sacral regions from the kidneys (6–9th weeks). The abnormal fusion of lower poles of kidneys during ascent form HSK.[5] Therefore, the index case presents a hypothesis that two simultaneously related events occurring during early organogenesis may be related. It will be interesting to know whether this was just incidental or there exists a true association.
The primary treatment for EGGCT is cisplatin-based chemotherapy followed by surgical resection of the residual tumor.[1] Cisplatin is known for inducing nephrotoxicity with dyselectrolytemia.[6] The degree of injury to the kidneys is dose dependent, and changes may persist for years after treatment. This has been abrogated by adequate pre-treatment hydration, chloride diuresis and administration of cisplatin in saline over 4–6 h. Carboplatin is an analogue of cisplatin developed as a less nephrotoxic alternative but was not found to be equipotent.[1] The standard of care, Bleomycin, Etoposide and Cisplatin (BEP), are more nephrotoxic and associated with pulmonary complications.[1] Patients with HSK are known to have renal problems affecting their function due to repeated infections and calculi.[5] As this was a case of mediastinal EGGCT and post-chemotherapy thoracic surgery was expected, BEP was avoided and TIP was used.[1,7] All precautions required during cisplatin therapy were taken in order to avoid renal injury. Serial monitoring of serum electrolytes and renal function show no abnormalities till date.
To summarize, our patient presents an unusual case of embryological association of mediastinal EGGCT with HSK and warrants future look out for such associations. It also highlights the important option of using TIP as primary chemotherapy in mediastinal EGGCT patients. Patients receiving nephrotoxic drugs should be managed cautiously with serial monitoring of renal functions and electrolytes.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared
REFERENCES
| Fig. 1 (a) Mediastinal mass at diagnosis, (b) Horseshoe kidney, (c) Mediastinal residual mass post chemotherapy, (d) Mediastinal recurrence post surgery