 PDF
PDF  Views
Views  Share
Share


Tongue trail to kidney
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2014; 35(01): 106-108
DOI: DOI: 10.4103/0971-5851.133735
Abstract
Renal cell carcinoma (RCC) has the propensity to metastasize to any organ in the body. Tongue metastases from RCC is very rare with most of them being metachronous in nature. We present a rare case where patient presented with a tongue lesion leading to a diagnosis of RCC. Surgery is the preferred modality of treatment for tongue metastases.
Publication History
Article published online:
19 July 2021
© 2014. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Renal cell carcinoma (RCC) has the propensity to metastasize to any organ in the body. Tongue metastases from RCC is very rare with most of them being metachronous in nature. We present a rare case where patient presented with a tongue lesion leading to a diagnosis of RCC. Surgery is the preferred modality of treatment for tongue metastases.
INTRODUCTION
Metastases comprise 0.2% of all tongue malignancies.[1] Lung and breast cancers are the most common to metastasize to the head and neck region, followed by renal cell carcinoma (RCC).[2] At this site, RCC metastases is usually of metachronous nature. Very few cases of tongue lesion leading to diagnosis of a renal primary have been reported in the literature.[2]
We present a rare case of tongue lesion as initial presentation of RCC.
CASE REPORT
This paper reports a case of a 63-year gentleman, chronic smoker, presented with progressively increasing swelling over dorsal surface of tongue with difficulty in swallowing for last 3 months. On examination a 3 × 3 cm superficial, mobile, pedunculated, proliferative growth was seen in midline of dorsal surface of tongue [Figure 1]. There was no palpable cervical adenopathy. A punch biopsy of the lesion suggested “carcinoma with clear cell morphology.” In view of histopathology, computed tomography (CT) scan of neck, chest and abdomen was done which revealed a 5 × 6 × 5 cm heterogeneously enhancing lesion in mid-region extending to upper pole of right kidney with multiple bilateral sub-centimeter lung nodules [Figure 2]. Fluoride positron emission tomography-CT done as a part of metastatic work-up did not reveal any other site of metastases.

| Figure 1:Image showing tongue metastases
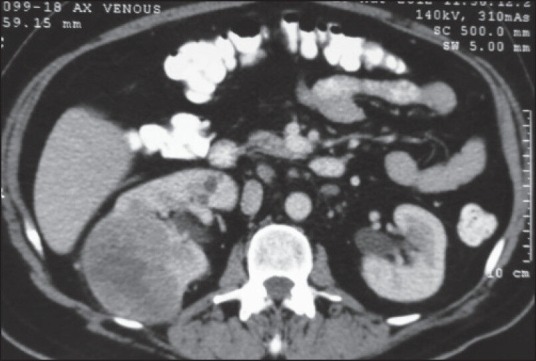
| Figure 2:Computed tomography scan showing right renal mass
Patient underwent right cytoreductive nephrectomy along with wide excision of tongue metastases. Tongue lesion was superficial and did not require any reconstruction. Lung lesions were small and multiple, and could not be resected. Histopathology of kidney mass confirmed the diagnosis of conventional clear cell carcinoma with Fuhrman's grade one (pT1bN0). Tongue histopathology was suggestive of metastatic deposits of clear cell RCC. Patient was started post-operatively on sunitinib in view of residual metastatic lung lesions.
DISCUSSION
RCC predominantly occurs in males (1.5:1) with peak incidence in the sixth decade. Approximately 30% of newly diagnosed RCC patients present with synchronous metastatic disease, and an additional 25-30% of patients with clinically localized disease eventually develop metastases. It can metastasize via lymphatic and hematogenous pathways to any location in the body. The common metastatic sites are lung, bone and liver.
Metastases in the head neck region from RCC are seen in 8-15% of patients with metastatic disease.[3] Most are metachronous in nature. Usually, it is a manifestation of widespread metastases in a known case of RCC, but at times such lesions can also lead to detection of a silent RCC. Primary localizing sites in the head neck region include paranasal sinuses, larynx, jaws, temporal bones, thyroid gland and parotid glands.[4] Lingual metastases represent only about 1% incidence of metastases to oral cavity and arise most commonly from melanomas, breast, gastrointestinal tract, lung and rarely from kidney.
From 1973 to 2011, 33 cases of a lingual metastasis of a primary kidney tumor were published in the English-language literature.[5] Until today, only 7 patients have presented primarily with tongue metastases leading to the diagnosis of RCC [Table 1].[2,6,7]
Table 1
Previous reports of metastasis of tongue

|
It has been postulated that in the absence of lung or liver lesions, the disease can spread through Batson's venous plexus or thoracic duct. Most tongue metastases involve the base due to its high vascularity and low mobility. However, our patient had a dorsal midline lesion in tongue.
Like primary tongue lesions, lingual metastases can be ulcerated or polypoid and tumor cells can infiltrate the muscle without involving the overlying mucosa.[1] Tomita et al. in their review of 18 cases of RCC with lingual metastases, considered this site to be associated with poor prognosis: 83.3% of cases had multiple metastases and mortality within 1 year was 67%.[8]
The rarity of this site of metastases can create a diagnostic dilemma in patients with clear cell histology. Malignant clear cell tumors of the head and neck arise as primary from the salivary, thyroid, or parathyroid glands and as secondaries from lung, female genital tract and kidney.
The treatment and best palliation of tongue metastases is surgical excision. Radiation therapy can aid in local symptom control with base tongue lesions.
Cytoreductive nephrectomy is justified in patients with metastatic disease to improve quality of life or local symptoms. Prospective trials have demonstrated that, in patients with synchronous metastatic disease, cytoreductive nephrectomy and cytokine therapy give a distinct survival advantage over immunotherapy alone.
Several retrospective studies have suggested that patients undergoing complete resection of limited metastatic foci may experience long disease free intervals, with median 5 year survival rate of 35-50% in some reports.[9] In a report by Kyan and Kato, surgical resection of lingual metastases followed by administration of interferon-alpha and interleukin-II had a disease free interval of 2 years.[10]
Many prospective trials have shown a prolongation of progression free survival and higher response rates with targeted molecular therapy in metastatic disease.
CONCLUSION
Tongue is a rare site for RCC metastases and in very few patients it has led to detection of an otherwise silent RCC. Only 7 such cases have been reported in the literature. The diagnosis is challenging for both the clinician and the pathologist. Renal evaluation for primary should be considered in differential diagnosis of tongue lesion with clear cell histology. Surgery is the preferred modality for treatment. Patients can achieve long disease free survival with combination of surgical excision and molecular therapy.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Zegarelli DJ, Tsukada Y, Pickren JW, Greene GW Jr. Metastatic tumor to the tongue. Report of twelve cases. Oral Surg Oral Med Oral Pathol 1973;35:202-11.
- Azam F, Abubakerr M, Gollins S. Tongue metastasis as an initial presentation of renal cell carcinoma: A case report and literature review. J Med Case Rep 2008;2:249.
- Pritchyk KM, Schiff BA, Newkirk KA, Krowiak E, Deeb ZE. Metastatic renal cell carcinoma to the head and neck. Laryngoscope 2002;112:1598-602.
- Som PM, Norton KI, Shugar JM, Reede DL, Norton L, Biller HF, et al. Metastatic hypernephroma to the head and neck. AJNR Am J Neuroradiol 1987;8:1103-6.
- Novak P, Sükösd F, Hamar S, Nemeth I, Tiszlavicz L, Szalay I, et al. Metachronous clear cell carcinoma of the tongue and kidney: A diagnostically challenging coincidence. Oral Surg Oral Med Oral Pathol Oral Radiol 2012;114:e25-30.
- Deniz A, Demet E, Ayca T, Umit B, Volkan B, Isin G, et al. Metastatic renal cell carcinoma initially presented as a tongue mass. Turk J Pathol 2010;26:261-3.
- Yoshitomi I, Kawasaki G, Mizuno A, Nishikido M, Hayashi T, Fujita S, et al. Lingual metastasis as an initial presentation of renal cell carcinoma. Med Oncol 2011;28:1389-94.
- Tomita T, Inouye T, Shinden S, Ogawa K, Mukai M. Palliative radiotherapy for lingual metastasis of renal cell carcinoma. Auris Nasus Larynx 1998;25:209-14.
- Russo P, Synder M, Vickers A, Kondagunta V, Motzer R. Cytoreductive nephrectomy and nephrectomy/complete metastasectomy for metastatic renal cancer. Scientific World Journal 2007;7:768-78.
- Kyan A, Kato SN. Renal cell carcinoma metastatic to the base of tongue: A case report. Hinyokika Kiyo 2004;50:791-3.
- Kapoor VK, Mukhopadhyay AK, Chattopadhyay TK, Sharma LK. Renal cell carcinoma metastatic to the tongue. J Indian Med Assoc 1987;85:119-20.
- Ziyada WF, Brookes JD, Penman HG. Expectorated tissue leading to diagnosis of renal adenocarcinoma. J Laryngol Otol 1994;108:1108-10.
- Aguirre A, Rinaggio J. Lingual metastasis of renal cell carcinoma. J Oral Maxillofac Surg 1996;54:344-6.
| Figure 1:Image showing tongue metastases
| Figure 2:Computed tomography scan showing right renal mass
References
- Zegarelli DJ, Tsukada Y, Pickren JW, Greene GW Jr. Metastatic tumor to the tongue. Report of twelve cases. Oral Surg Oral Med Oral Pathol 1973;35:202-11.
- Azam F, Abubakerr M, Gollins S. Tongue metastasis as an initial presentation of renal cell carcinoma: A case report and literature review. J Med Case Rep 2008;2:249.
- Pritchyk KM, Schiff BA, Newkirk KA, Krowiak E, Deeb ZE. Metastatic renal cell carcinoma to the head and neck. Laryngoscope 2002;112:1598-602.
- Som PM, Norton KI, Shugar JM, Reede DL, Norton L, Biller HF, et al. Metastatic hypernephroma to the head and neck. AJNR Am J Neuroradiol 1987;8:1103-6.
- Novak P, Sükösd F, Hamar S, Nemeth I, Tiszlavicz L, Szalay I, et al. Metachronous clear cell carcinoma of the tongue and kidney: A diagnostically challenging coincidence. Oral Surg Oral Med Oral Pathol Oral Radiol 2012;114:e25-30.
- Deniz A, Demet E, Ayca T, Umit B, Volkan B, Isin G, et al. Metastatic renal cell carcinoma initially presented as a tongue mass. Turk J Pathol 2010;26:261-3.
- Yoshitomi I, Kawasaki G, Mizuno A, Nishikido M, Hayashi T, Fujita S, et al. Lingual metastasis as an initial presentation of renal cell carcinoma. Med Oncol 2011;28:1389-94.
- Tomita T, Inouye T, Shinden S, Ogawa K, Mukai M. Palliative radiotherapy for lingual metastasis of renal cell carcinoma. Auris Nasus Larynx 1998;25:209-14.
- Russo P, Synder M, Vickers A, Kondagunta V, Motzer R. Cytoreductive nephrectomy and nephrectomy/complete metastasectomy for metastatic renal cancer. Scientific World Journal 2007;7:768-78.
- Kyan A, Kato SN. Renal cell carcinoma metastatic to the base of tongue: A case report. Hinyokika Kiyo 2004;50:791-3.
- Kapoor VK, Mukhopadhyay AK, Chattopadhyay TK, Sharma LK. Renal cell carcinoma metastatic to the tongue. J Indian Med Assoc 1987;85:119-20.
- Ziyada WF, Brookes JD, Penman HG. Expectorated tissue leading to diagnosis of renal adenocarcinoma. J Laryngol Otol 1994;108:1108-10.
- Aguirre A, Rinaggio J. Lingual metastasis of renal cell carcinoma. J Oral Maxillofac Surg 1996;54:344-6.