 PDF
PDF  Views
Views  Share
Share


The changing nature of end of life care
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2015; 36(02): 94-98
DOI: DOI: 10.4103/0971-5851.158836
Abstract
Good end of life care (EOLC) for patients with incurable cancer is becoming a greater priority for oncologists in recent years. Frameworks such as the Liverpool Care Pathway (LCP) have often been helpful in guiding good care at the end of life. However, in the past year, the LCP has been phased out of use in the United Kingdom (UK), following concerns that it was poorly implemented. This review describes the LCP′s origins in the UK, its strengths and limitations, and the concerns that prompted a review of its use. It describes the recommendations for change made by an independent review, and the alternative strategies now being developed in the UK to guide good EOLC. Although the LCP is still being widely used worldwide, the lessons learned from the UK can be widely applied in other countries.
Publication History
Article published online:
12 July 2021
© 2015. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Good end of life care (EOLC) for patients with incurable cancer is becoming a greater priority for oncologists in recent years. Frameworks such as the Liverpool Care Pathway (LCP) have often been helpful in guiding good care at the end of life. However, in the past year, the LCP has been phased out of use in the United Kingdom (UK), following concerns that it was poorly implemented. This review describes the LCP's origins in the UK, its strengths and limitations, and the concerns that prompted a review of its use. It describes the recommendations for change made by an independent review, and the alternative strategies now being developed in the UK to guide good EOLC. Although the LCP is still being widely used worldwide, the lessons learned from the UK can be widely applied in other countries.
INTRODUCTION
The importance of good end of life care (EOLC) in India has been highlighted in recent months, with one million new cancer cases diagnosed each year, expected to rise five-fold by 2025.[1] A recent international study of “quality of death” ranked India the lowest of 40 countries in the EOLC overall score.[2] Recent guidelines from the Indian Journal of Critical Care Medicine,[3] and the Indian Association of Palliative Care position statement[4] have aimed to address this issue. They have highlighted that there are several barriers to good EOLC in India: Insufficient number of doctors with appropriate training, lack of laws governing resuscitation orders, and patient and family expectations about active treatment, being just some.
However, in continuing to treat cancer patients approaching the end of life, there are both financial implications for families paying for burdensome treatment, as well as an impact on patients’ experiences at the end of life. EOLC pathways have been developed to help guide nonpalliative care professionals to care for patients at the end of life. Worldwide, the most commonly used pathway is the Liverpool Care Pathway (LCP). However in recent months, concerns about its implementation were raised, leading to an independent review chaired by Baroness Julia Neuberger and a subsequent recommendation for its withdrawal in the United Kingdom (UK).[5]
This review describes the history of the LCP, the events surrounding its withdrawal from use in the UK, and the subsequent recommendations for change made following the Neuberger review. It also looks at the evidence for using EOLC pathways, highlighting the importance of these tools, as well as their limitations.
HISTORY OF THE LIVERPOOL CARE PATHWAY
Not all dying patients have access to, or indeed need, specialist palliative care services; the majority of patients are cared for by nonspecialists. As such in the late 1990s, the LCP was developed in the UK, by palliative care specialists at the Royal Liverpool University Hospital, working in conjunction with the Marie Curie Palliative Care Institute. Its aim was to transfer the “gold standard” excellence of care patients received at the end of life in a hospice, to all settings. This would ensure that patients in the final few days and hours of life received the best possible care, whether they were at home, in a hospice, nursing home or hospital.
The pathway was intended to guide good care to allow as dignified and peaceful death as possible, using a patient-centered and holistic approach. It prompted the healthcare professional (in consultation with the patient and/or the family) to make decisions about appropriate ceilings of care. This included prompts about the continued appropriateness of monitoring vital signs, blood tests, medications, the need (or otherwise) for artificial hydration and nutrition, and cardiopulmonary resuscitation status. The LCP did not dictate that these interventions necessarily needed to be ceased. It guided healthcare professionals to make regular assessments of the patient's comfort, and to act upon any symptoms that occurred. Finally, it highlighted the importance of considering not just the physical aspect of their illness, but also the psychological, social and spiritual elements. This translated, for example, to ensure that communication with patients, and if appropriate, their families, was prioritized.[6,7] Of note, the LCP was not intended to be a treatment in itself, but a guide to best practice. Over the following decade, the use of the LCP extended outside the UK, to countries such as India, Italy, Norway, and New Zealand.
EVIDENCE FOR THE LIVERPOOL CARE PATHWAY
When the LCP was initially developed and rolled out, there was no robust research evidence suggesting that EOLC pathways improved outcomes for patients or their families.
In 2013, the Cochrane database published an updated version of their 2010 review assessing the effects of EOLC pathways, compared with usual practice (i.e., no pathway) across all healthcare settings. It particularly aimed to assess the effects on symptom severity and quality of life of people who are dying, as well as the impact on care for families, carers, and health professionals. The review included randomized controlled trials, quasi-randomized trials, or high quality before-and-after studies comparing the use versus nonuse of an EOLC pathway for the dying. The 2010 review identified 920, and the 2013 review an additional 1122, potentially relevant titles. None of these met the inclusion criteria, and so the review concluded that there was insufficient evidence available to recommend, or not recommend, the use of care pathways at the end of life. It went on to advise that all health services using EOLC pathways should independently audit their use, and subsequent use of pathways should be based on carefully documented evaluations.[8]
Subsequently, in 2014, Costantini et al. published a cluster randomized trial assessing the effectiveness of the LCP in Italy (LCP-I) in improving the EOLC for patients with cancer in the hospital and their families. Sixteen Italian general medical hospital wards were randomized to implement the LCP-I program or standard practice. For each ward, all patients who died from cancer 3 months before and in the 6 months after completion of the LCP-I training program were identified. The primary endpoint assessed the overall quality of care, based on the quality of care toolkit scale. Following the implementation of the program, family members observed no significant difference in the overall quality of care scale between the two groups. However, a significant difference was observed for two secondary endpoints: Compared to the standard practice group the intervention group showed a better score in the “respect, dignity, and kindness” scale, and an improvement in the control of breathlessness. In addition, the study showed no adverse consequences of being on an EOLC pathway. The authors concluded that this trial suggested that when carefully implemented, EOLC pathways have the potential to narrow the gap between hospice and hospital care standards at the end of life.[9]
THE DEMISE OF THE LIVERPOOL CARE PATHWAY IN THE UNITED KINGDOM
Despite the promising research into the effect of the LCP on standards of care at the end of life, the LCP was not universally praised in the UK press, by patients and families, or by health care professionals.
In 2009, the Daily Telegraph (a national UK newspaper) wrote that the pathway had been blamed by some doctors for hastening the death of terminally ill patients, and possibly masking signs that patients were improving.[10] Furthermore, in 2012 and 2013, the LCP was more heavily criticized in the media, being dubbed a “death pathway” which was not discussed with patients or their families, and which often involved withdrawal of nutrition and hydration. Several cases were highlighted in which patients had been placed on the LCP and then went on to make a full recovery.[11] On the whole, this was interpreted by the media to indicate that the LCP had been responsible for the patient's deterioration and that removal from the pathway had led to recovery. The alternative possibility that recovering patients were removed from the LCP as their condition improved was rarely discussed. In addition, in many National Health Service (NHS) trusts, use of the LCP was attached to financial incentives, known as Commissioning for Quality and Innovation payments. Although the intention of these incentives had been to encourage the use of the LCP, as part of best practice, the media portrayed a situation in which a possibly “lethal” tool was being used as part of a money-making system for trusts.[12]
Furthermore, it was reported that not all health care professionals supported the use of the LCP. For example, in October 2012 the Daily Mail, a widely read national newspaper in the UK, wrote that the LCP was “a pathway to killing people that doctors deem worthless.”[13] Articles such as these caused a significant breakdown of trust in the LCP, for patients, their families and nonspecialist health care professionals.
THE NEUBERGER REVIEW
Following the widespread media criticism of the LCP, Norman Lamb, the government Minister of State for Care Support, ordered an independent review of the LCP to be carried out, examining the use and experience of the LCP in England. This was chaired by rabbi and peer Julia Neuberger, and was separate from the NHS and government.
The review considered evidence from different sources: From members of the public and health care professionals who had experience of the LCP, as well as professional bodies. A review of academic literature and relevant hospital complaints, and surveys of health care professionals were also considered. In July 2013, the review's findings were published in a report entitled More Care Less Pathway[5]. It found that many relatives of people dying whilst being treated under the LCP felt that their loved ones had had good deaths, and that if the LCP was used appropriately, by well-trained, resourced, and sensitive clinical teams, it worked well. However, it also highlighted several areas of concern.
First, the review noted that it is hard to accurately judge when someone is dying, and therefore in the wrong hands, the LCP had the potential to be used inappropriately. The LCP was designed as a tool to help guide best care in the patient's last few days and hours of life, including rationalizing burdensome treatments that would not alter the outcome. The report uncovered examples of health care professionals displaying a lack of understanding about the difference between palliative and terminal care, with the risk that the LCP could be commenced too early in palliative patients who were not imminently dying. In addition the term “pathway” was criticized, for giving the impression to some families that a decision had been made to hasten the death of their loved one by stopping all life-prolonging treatment, and that death was inevitable. Concerns were raised that in some cases the LCP became a “tick box” exercise, so that the LCP in itself became the treatment, as opposed to guiding best practice alongside assessing each patient's needs individually.
Problems with poor communication between healthcare professionals and patients and their families were at the heart of the review. It was felt that when patients had capacity to make decisions about their treatment, they were often not involved in discussions about starting the LCP, stopping artificial nutrition and hydration, stopping nonessential medications, not offering cardiopulmonary resuscitation in the event of a cardiorespiratory arrest, or using strong pain killing or sedatives. Once patients lost capacity, often families felt they were not included in discussions, and sometimes felt “railroaded” into agreeing to the cessation of certain treatments and starting the LCP. Finally, the review noted wider problems including reports of a lack of care and compassion shown to patients being treated on the LCP, often due to staff shortages and lack of training.
The report made several recommendations for change. It advised that the LCP should be phased out, over a period of 6-12 months, and replaced with an individual EOLC plan for each patient. It also called for an increase in research into better prognostic tools and more evidence on the use of sedation and strong analgesia at the end of life. It recommended more training to support healthcare professionals to care for patients at the end of life and to improve communication with their relatives and carers. The review stated that, where possible, patients should be placed on an end of life plan by the senior responsible clinician, and that this decision ought to be taken in working hours following discussion with the patient if possible, and/or their relatives. In addition, it called for an end to financial incentives for use of the LCP, or similar approaches. Finally, it recommended the initiation of an urgent system-wide approach to improving EOLC, working with professional bodies to issue guidance to their members, with ongoing assessments of the quality of EOLC.
THE LEADERSHIP ALLIANCE FOR THE CARE OF DYING PEOPLE
The Leadership Alliance for the Care of Dying People, made up of 21 national health and care organizations, was formed in order to respond to the recommendations set out in More Care, Less Pathway. The alliance included representation from professional bodies, the Department of Health, the Care Quality Commission and palliative care charities. Their response, One Chance to Get it Right, was published in June 2014.[14]
They recommended that five priorities of care be considered when caring for a patient who is thought to be in the final few days or hours of life [Box 1].
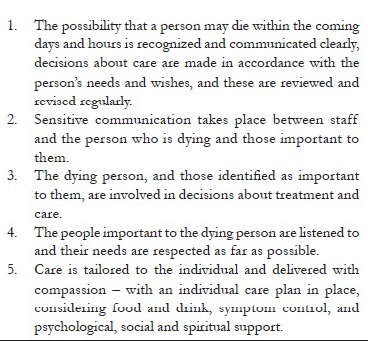
| Box 1 Priorities of care suggested by One Chance to Get it Right[14]
These priorities put patients and their loved ones at the heart of decisions about their treatment. Alliance members committed to these principles, in each of their roles, from initial training to inspection, and the initial responses from government, medical and nursing professional bodies, and Baroness Neuberger were positive.[15]
Since June 2014 the LCP is no longer in use in the UK. However, trusts have been developing alternative models of care, such as the Amber Care Bundle, developed at Guys and St Thomas’ Hospitals.[16] This approach identifies patients who may not recover from their current illness, but for whom active treatment is currently continuing. It prompts clinicians to openly discuss the possibility that the patient may not recover so that appropriate ceilings of care are set, and so that patients can discuss their wishes about their care should they not improve.
RESPONSE TO THE DEMISE OF THE LIVERPOOL CARE PATHWAY AND THE FUTURE
Following the Neuberger review and its recommendations, there seemed little doubt that the LCP had to be replaced. However, its withdrawal from use was not universally supported. Some palliative care professionals were concerned that a good tool had been phased out because of poor implementation, surmising that it was those using it, and not the tool itself, who were at fault.[7,17] In addition, concerns have been raised that although the LCP had little research supporting its implementation initially neither do the new recommendations.
The LCP debate has highlighted a number of important issues. It has raised the profile of palliative care, calling for a focus on new research to ascertain how people are best cared for at the end of life, and training to ensure that nonspecialists have the knowledge and attitudes required to provide good EOLC.
It has also emphasized the importance of more openly discussing death as a society and as medical professionals. As long as the taboo surrounding discussions about death remains, it will be challenging for medicine as a whole to provide patients with the compassionate, high-quality care that permits a comfortable and dignified death.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
| Box 1 Priorities of care suggested by One Chance to Get it Right[14]