 PDF
PDF  Views
Views  Share
Share


Sociodemographic Factors and Late stage Diagnosis of Breast Cancer in India: A Hospital based Study
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(03): 277-281
DOI: DOI: 10.4103/ijmpo.ijmpo_15_16
Abstract
Context: Breast cancer (BC) is one of the major causes of cancer mortality in India. Late-stage diagnosis of BC is associated with poor survival. Identification of factors affecting late presentation of the disease could be an effective step to reduce BC mortality. Aims: To study the association of sociodemographic factors with BC stage at diagnosis. Settings and Design: The study is a retrospective analysis from the case records from a single institution. Subjects and Methods: Data for the year 2008 was collected from the hospital records. A total of 1210 cases were included for the analysis. Sociodemographic factors included were age, place of residence, religion, marital status, level of education, and occupation. Other study variables were family history, presence of comorbidity, and stage at diagnosis. Statistical Analysis: Association between sociodemographic factors by stage at diagnosis was tested using Chi-square statistics, with odds ratios (ORs) estimated through logistic regression modeling. Results: In the study cohort, 46% patients had reported at early stages and 54% at advanced stages. All factors were evaluated for being predictors of disease stage at presentation using univariate and multivariate logistic regression model. Women from urban background were less likely to present with advanced stage disease (OR = 0.64; 95% confidence interval [CI]: 0.49–0.84) as compared to rural women. Similarly, illiterate women were also more likely to present with advanced-stage disease (OR = 1.55; 95% CI: 1.16–2.09). Conclusions: This data clearly indicate that the patients of rural background and of low education status are more likely than their respective counterparts to have an advanced stage of BC diagnosis. Our results may be considered the keys to determining how stage variation may be related to patients and community characteristics and where limited resources need to be invested to ensure early diagnosis of BC.
Publication History
Article published online:
04 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Context:
Breast cancer (BC) is one of the major causes of cancer mortality in India. Late-stage diagnosis of BC is associated with poor survival. Identification of factors affecting late presentation of the disease could be an effective step to reduce BC mortality.
Aims:
To study the association of sociodemographic factors with BC stage at diagnosis.
Settings and Design:
The study is a retrospective analysis from the case records from a single institution.
Subjects and Methods:
Data for the year 2008 was collected from the hospital records. A total of 1210 cases were included for the analysis. Sociodemographic factors included were age, place of residence, religion, marital status, level of education, and occupation. Other study variables were family history, presence of comorbidity, and stage at diagnosis.
Statistical Analysis:
Association between sociodemographic factors by stage at diagnosis was tested using Chi-square statistics, with odds ratios (ORs) estimated through logistic regression modeling.
Results:
In the study cohort, 46% patients had reported at early stages and 54% at advanced stages. All factors were evaluated for being predictors of disease stage at presentation using univariate and multivariate logistic regression model. Women from urban background were less likely to present with advanced stage disease (OR = 0.64; 95% confidence interval [CI]: 0.49–0.84) as compared to rural women. Similarly, illiterate women were also more likely to present with advanced-stage disease (OR = 1.55; 95% CI: 1.16–2.09).
Conclusions:
This data clearly indicate that the patients of rural background and of low education status are more likely than their respective counterparts to have an advanced stage of BC diagnosis. Our results may be considered the keys to determining how stage variation may be related to patients and community characteristics and where limited resources need to be invested to ensure early diagnosis of BC.
Breast cancer (BC) is the most frequently diagnosed cancer and the leading cause of cancer-related death among women worldwide. The annual age-standardized incidence rate of BC worldwide in 2012 was 43.1/100,000 women and 25.8/100,000 in India.[1] However, despite a lower incidence the BC mortality in India (12.7/100,000) is similar to worldwide mortality (12.9/100,000).[2] Within India also, there are substantial differences in BC incidence rates between rural and urban areas. rates observed in urban registries range from 29/100,000 to 35/100,000 women, whereas those observed in rural registries vary from 10/100,000 to 12/100,000 women.[3] BC is said to be most common cancer in females of urban India. The rise of BC in India is a cause for concern and calls for increased awareness of factors associated with the disease.[4] A low level of awareness and knowledge about BC has been found to be associated with delayed presentation.[5] Epidemiologic evidence exists that late-stage diagnosis for BC is related to a number of sociodemographic factors such as age, level of education, marital status, unemployment, and family history of BC.[6,7,8,9] Long-term prognosis of BC patients strongly depends on stage of disease at diagnosis.[10] The 5-year survival rates of patients treated for carcinoma of the breast are dependent on the stage of diagnosis with a survival of 100% in patients with Stage 0 and Stage I disease.[11] Detecting new BCs in its earliest stages increases the probability of long-term survival, which is why early disease detection is of the utmost importance.[12]
There are few studies in India that have examined the influence of sociodemographic factors on late presentation among BC patients. It is, therefore, desirable to assess the effect of these factors on late reporting. Findings of which may assist in developing appropriate strategies aimed at reducing delay. Therefore, this study was aimed to examine the association and impact of sociodemographic factors on the stage at diagnosis of BC patients in India.
Study design
This study design is based on retrospective BC data collected from the Hospital-Based Cancer Registry, Tata Memorial Hospital (TMH), Mumbai, India.
Study population
BC patients were included in the present study if they had reported in the year 2008 and taken the treatment in TMH (n = 1210). Patients were excluded if they had undergone any cancer-directed treatment elsewhere before reporting at the TMH.
Data collection
Data were retrospectively abstracted and analyzed from the hospital electronic medical records system. Sociodemographic factors and other background variables recorded are age (below 49 years vs. 49 and above), place of residence (rural/urban), religion (Hindu, Muslim, or others), marital status (married, widow/divorced, unmarried), level of education (illiterate, literate/primary, secondary, and college and above), and occupation (working and nonworking). Other study variables were family history of cancer (yes/no), presence of comorbidity, and stage at diagnosis (Stages I and II were identified as “early” and III and IV as “advanced”).
Statistical analysis
Association between sociodemographic factors by stage at diagnosis was tested using Chi-square statistics. The odds ratios (ORs) for late-stage reporting and their 95% confidence intervals (CIs) according to sociodemographic factors were estimated through logistic regression model. All the analyses were done using the statistical package SPSS software v20.0 (SPSS, IBM, Chicago, IL).
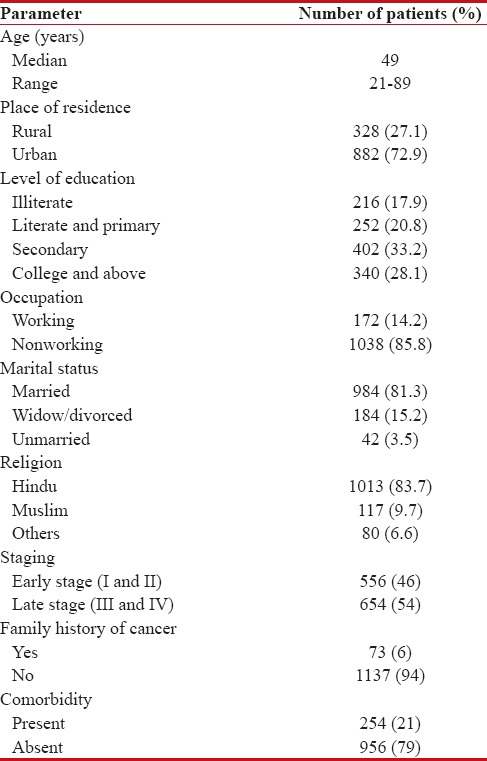
A total of 2112 BC patients registered at the TMH during the year 2008. Nine-hundred and two patients who had undergone partial treatment before reporting to the TMH were excluded from the present analysis. The total number of patients analyzed was 1210. Age of patients ranged from 21 to 89 years with a mean age of 49 years. Twenty-seven percent of patients were found to be resident of rural area and 73% of population from urban area. Patients belonging to the Hindu faith constituted 83.7%, Muslims 9.7%, and others 6.6%. Eighty-one percent of patients were married, 15.2%-widowed or divorced, and 3.5%-were unmarried. Eighteen percent of patients were illiterate, and 28.1%-had higher education of college and above. Only fourteen percent of patients reported to be employed or working [Table 1].
Table 1
Patient's characteristics
|
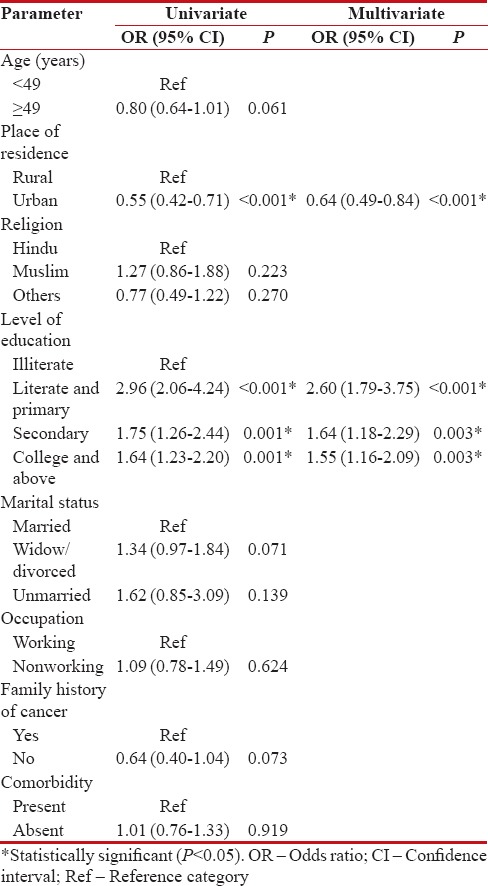
Table 2 describes the various sociodemographic factors and their relationship to the stage at diagnosis. Forty-six percent were diagnosed at an “early” stage of BC and 54%-were diagnosed at a “late” stage. Age at the time of diagnosis, place of residence, religion, marital status, level of education, and occupation were evaluated for being predictors of disease stage at presentation using univariate and multivariate logistic regression model. Women from urban background were less likely to present with advanced-stage disease (OR = 0.64; 95%-CI: 0.49–0.84) as compared to rural women. Similarly, illiterate women were also more likely to present with advanced stage disease (OR = 1.55; 95%-CI: 1.16–2.09). All the other factors were not found to be significantly associated with stage at presentation.
Table 2
Univariate and multivariate analysis of sociodemographic factors by late stage of breast cancer patients
|
Discussion
India is a vast country with varying social, cultural, and religious practices. Cultural dynamics and sociodemographic differences across population subgroups modulate how biologic disease is expressed among different ethnic groups.[13] These interactions contribute to the observed variations in breast carcinoma incidence, mortality, and survival. Stage, a measure of disease status, is used to assess prognosis, plan treatment, and evaluate outcome. Long-term prognosis of BC patients strongly depends on stage of disease at diagnosis.[14] Factors associated with advanced stage at diagnosis in multicultural populations range from changes in the basic biological characteristics at the molecular and cellular level to societal issues – such as access to care and socioeconomic conditions – all of which impact on the health measure called “stage at diagnosis.”[13] BC in developing countries is characterized by late presentation, advanced stage of disease at diagnosis, worse biologic behavior, and occurrence in younger women than reported in the developed countries.[15]
The present study analyzed the impact of sociodemographic factors according to the stage at diagnosis among BC patients reporting to a major cancer hospital in India. Our study findings found that 54%-of the patients presented with an advanced stages of cancer. Such high proportion of late-stage presentation is a reflection of the cultural norms which downplay women's health problems.[16]
BC is more probable to be diagnosed at earlier stages in urban women than in rural women and consequently more treatable.[17] In this study, the relationship between late stage at diagnosis and living in rural background was significant (P < 0 xss=removed>et al., living place has an important role in defining risk of advanced BC.[18] Former studies have also reported that late stage at diagnosis and lower survival have been linked to poor access to healthcare facilities and lower awareness, especially in the urban poor and rural populations as well as demographic factors such as lower education and literacy.[9,19] Harirchi et al. in their study found that living in small cities and lack of access to health-care systems and health facilities contribute to delay in referring patients with advanced level of BC.[20] There are multiple factors that delay diagnosis in Indian women, ranging from limited availability and access to cancer health services, lower health literacy, and social stigma.[21]
In our study, we found that education played a significant role in the diagnosis of the BC. In other words, those with lower educational level were referred at more advanced level of disease. Education is a key factor of the socioeconomic status, which influences lifestyles, behavioral patterns, reproductive factors, such as parity and even stage at presentation.[22] Socioeconomic status has massive influence on a woman's health. Women with low socioeconomic status are more likely to be diagnosed with advanced BC compared to more economically privileged women.[23] A low level of education and a low socioeconomic status lead to poor uptake of screening by women. Previous studies have demonstrated that lower education and income are the most important causes of delay in diagnosis of BC in women in the developing countries.[9,20,21,22,23,24] Harirchi et al. have also reported that lower education is one of the most important causes of delay in referring to practitioners with advanced level of cancer.[20] Similarly, Richardson et al. also reported low socioeconomic status is one of the risk factors of late-stage diagnosis of BC and patients' referring.[25]
In the present study, 52%-of younger women (<49>49 years) presented with late disease. Although there are many studies in literature which have found that older women are more likely to present with late-stage BC, our study failed to find this association. Similarly, Satariano and Ragland in their study of 936 BC patients failed to find any statistical association between age and stage of disease.[26] This may be due to similar average age in both early- and late-stage group of patients. The present study also did not find any association between presence of comorbidity and stage of diagnosis, which is similar to results reported earlier by other studies.[27,28] A systematic review conducted by Ramirez et al.[29] in 1999 found strong evidence that marital status was unrelated to delays by patients in reporting the disease, which is similar to our study. In the present study, family history of BC was not associated with stage at diagnosis as did by Burgess et al.[30] and Meechan et al.[31] Yip et al. reported no difference in size, stage, and duration of symptoms of BC between Malaysian women with a positive family history and those without.[32] Thus, the finding of the current study further emphasizes that specific factors are of particular importance in certain groups of patients and vice versa. Investigation and better understanding the nature of the BC-related health beliefs and attitudes of the general female population hold the key to reduce late-stage presentation of BC. Hence, an explicit, comprehensive model of human emotions, cognitions, and behaviors is required as the basis for assessment of the psychosocial risk factors.
This study has examined a range of individual factors that might influence BC stage at the time of diagnosis. To our knowledge, this work is unique in looking at sociodemographic factors in a hospital-based sample of BC patients. However, our study is not devoid limitations and hence must be considered while interpreting the results. One of the main limitations is that we could not consider the major sociodemographic factor such as income in our study as it was not documented at the time of registration in the hospital.
BC being the leading cause of death due to malignant neoplasm in the female population worldwide is currently a public health problem which merits priority attention. This study may represent a contribution to the investigation of the factors associated with later stage BC diagnoses in India. Our results may be considered the keys to determining how stage variation may be related to patients and community characteristics and where to invest limited resources for ensuring an early diagnosis and treatment of BC.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC Cancer Base No. 11. Lyon, France: International Agency for Research on Cancer; 2013. Available from: http://www.globocan.iarc.fr. [Last accessed on 2016 Jan 24].
- Rajaraman P, Anderson BO, Basu P, Belinson JL, Cruz AD, Dhillon PK, et al. Recommendations for screening and early detection of common cancers in India. Lancet Oncol 2015;16:e352-61.
- Nagrani RT, Budukh A, Koyande S, Panse NS, Mhatre SS, Badwe R, et al. Rural urban differences in breast cancer in India. Indian J Cancer 2014;51:277-81.
- Curado MP, Edwards B, Shin HR, Storm H, Ferlay J, Heanue M, et al. Cancer Incidence in Five Continents. IARC Scientific Publications No. 160. Vol. IX. Lyon, France: IARC; 2007.
- Agarwal G, Ramakant P. Breast cancer care in India: The current scenario and the challenges for the future. Breast Care (Basel) 2008;3:21-7.
- Kaffashian F, Godward S, Davies T, Solomon L, McCann J, Duffy SW, et al. Socioeconomic effects on breast cancer survival: Proportion attributable to stage and morphology. Br J Cancer 2003;89:1693-6.
- Stavraky KM, Skillings JR, Stitt LW, Gwadry-Sridhar F. The effect of socioeconomic status on the long-term outcome of cancer. J Clin Epidemiol 1996;49:1155-60.
- Dalton SO, Ross L, Düring M, Carlsen K, Mortensen PB, Lynch J, et al. Influence of socioeconomic factors on survival after breast cancer – A nationwide cohort study of women diagnosed with breast cancer in Denmark 1983-1999. Int J Cancer 2007;121:2524-31.
- Ali R, Mathew A, Rajan B. Effects of socio-economic and demographic factors in delayed reporting and late-stage presentation among patients with breast cancer in a major cancer hospital in South India. Asian Pac J Cancer Prev 2008;9:703-7.
- Yabroff KR, Gordis L. Does stage at diagnosis influence the observed relationship between socioeconomic status and breast cancer incidence, case-fatality, and mortality? Soc Sci Med 2003;57:2265-79.
- American Cancer Society. Breast Cancer Survival Rates by Stage. Available from: http://www.cancer.org/cancer/breastcancer/detailedguide/breast-cancer-survival-by-stage. [Last accessed on 2016 Jan 12].
- Hanrahan EO, Gonzalez-Angulo AM, Giordano SH, Rouzier R, Broglio KR, Hortobagyi GN, et al. Overall survival and cause-specific mortality of patients with stage T1a, bN0M0 breast carcinoma. J Clin Oncol 2007;25:4952-60.
- Herndon JE 2nd, Kornblith AB, Holland JC, Paskett ED. Effect of socioeconomic status as measured by education level on survival in breast cancer clinical trials. Psychooncology 2013;22:315-23.
- Hunter CP. Epidemiology, stage at diagnosis, and tumor biology of breast carcinoma in multiracial and multiethnic populations. Cancer 2000;88:1193-202.
- Memon ZA, Shaikh AN, Rizwan S, Sardar MB. Reasons for patient's delay in diagnosis of breast carcinoma in Pakistan. Asian Pac J Cancer Prev 2013;14:7409-14.
- Miller AB. Mammography: A critical evaluation of its role in breast cancer screening, especially in developing countries. J Public Health Policy 1989;10:486-98.
- Babu GR, Lakshmi SB, Thiyagarajan JA. Epidemiological correlates of breast cancer in south India. Asian Pac J Cancer Prev 2013;14:5077-83.
- MacKinnon JA, Duncan RC, Huang Y, Lee DJ, Fleming LE, Voti L, et al. Detecting an association between socioeconomic status and late stage breast cancer using spatial analysis and area-based measures. Cancer Epidemiol Biomarkers Prev 2007;16:756-62.
- Sharma K, Costas A, Shulman LN, Meara JG. A systematic review of barriers to breast cancer care in developing countries resulting in delayed patient presentation. J Oncol 2012;2012:121873.
- Harirchi I, Ghaemmaghami F, Karbakhsh M, Moghimi R, Mazaherie H. Patient delay in women presenting with advanced breast cancer: An Iranian study. Public Health 2005;119:885-91.
- Leong SP, Shen ZZ, Liu TJ, Agarwal G, Tajima T, Paik NS, et al. Is breast cancer the same disease in Asian and western countries? World J Surg 2010;34:2308-24.
- Gadgil A, Roy N, Sankaranarayanan R, Muwonge R, Sauvaget C. Effect of comprehensive breast care on breast cancer outcomes: A community hospital based study from Mumbai, India. Asian Pac J Cancer Prev 2012;13:1105-9.
- Miller BA, Hankey BF, Thomas TL. Impact of sociodemographic factors, hormone receptor status, and tumor grade on ethnic differences in tumor stage and size for breast cancer in US women. Am J Epidemiol 2002;155:534-45.
- Mohaghegh P, Yavari P, Akbari ME, Abadi A, Ahmadi F. Associations of demographic and socioeconomic factors with stage at diagnosis of breast cancer. Asian Pac J Cancer Prev 2015;16:1627-31.
- Richardson JL, Langholz B, Bernstein L, Burciaga C, Danley K, Ross RK, et al. Stage and delay in breast cancer diagnosis by race, socioeconomic status, age and year. Br J Cancer 1992;65:922-6.
- Satariano WA, Ragland DR. The effect of comorbidity on 3-year survival of women with primary breast cancer. Ann Intern Med 1994;120:104-10.
- Neal RD, Allgar VL. Sociodemographic factors and delays in the diagnosis of six cancers: Analysis of data from the “National survey of NHS patients: Cancer”. Br J Cancer 2005;92:1971-5.
- Meechan G, Collins J, Petrie K. Delay in seeking medical care for self-detected breast symptoms in New Zealand women. N Z Med J 2002;115:U257.
- Ramirez AJ, Westcombe AM, Burgess CC, Sutton S, Littlejohns P, Richards MA, et al. Factors predicting delayed presentation of symptomatic breast cancer: A systematic review. Lancet 1999;353:1127-31.
- Burgess CC, Ramirez AJ, Richards MA, Love SB. Who and what influences delayed presentation in breast cancer? Br J Cancer 1998;77:1343-8.
- Meechan G, Collins J, Petrie KJ. The relationship of symptoms and psychological factors to delay in seeking medical care for breast symptoms. Prev Med 2003;36:374-8.
- Yip CH, bt Mohd Taib NA, Lau PC. Does a positive family history influence the presentation of breast cancer? Asian Pac J Cancer Prev 2008;9:63-5.
References
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC Cancer Base No. 11. Lyon, France: International Agency for Research on Cancer; 2013. Available from: http://www.globocan.iarc.fr. [Last accessed on 2016 Jan 24].
- Rajaraman P, Anderson BO, Basu P, Belinson JL, Cruz AD, Dhillon PK, et al. Recommendations for screening and early detection of common cancers in India. Lancet Oncol 2015;16:e352-61.
- Nagrani RT, Budukh A, Koyande S, Panse NS, Mhatre SS, Badwe R, et al. Rural urban differences in breast cancer in India. Indian J Cancer 2014;51:277-81.
- Curado MP, Edwards B, Shin HR, Storm H, Ferlay J, Heanue M, et al. Cancer Incidence in Five Continents. IARC Scientific Publications No. 160. Vol. IX. Lyon, France: IARC; 2007.
- Agarwal G, Ramakant P. Breast cancer care in India: The current scenario and the challenges for the future. Breast Care (Basel) 2008;3:21-7.
- Kaffashian F, Godward S, Davies T, Solomon L, McCann J, Duffy SW, et al. Socioeconomic effects on breast cancer survival: Proportion attributable to stage and morphology. Br J Cancer 2003;89:1693-6.
- Stavraky KM, Skillings JR, Stitt LW, Gwadry-Sridhar F. The effect of socioeconomic status on the long-term outcome of cancer. J Clin Epidemiol 1996;49:1155-60.
- Dalton SO, Ross L, Düring M, Carlsen K, Mortensen PB, Lynch J, et al. Influence of socioeconomic factors on survival after breast cancer – A nationwide cohort study of women diagnosed with breast cancer in Denmark 1983-1999. Int J Cancer 2007;121:2524-31.
- Ali R, Mathew A, Rajan B. Effects of socio-economic and demographic factors in delayed reporting and late-stage presentation among patients with breast cancer in a major cancer hospital in South India. Asian Pac J Cancer Prev 2008;9:703-7.
- Yabroff KR, Gordis L. Does stage at diagnosis influence the observed relationship between socioeconomic status and breast cancer incidence, case-fatality, and mortality? Soc Sci Med 2003;57:2265-79.
- American Cancer Society. Breast Cancer Survival Rates by Stage. Available from: http://www.cancer.org/cancer/breastcancer/detailedguide/breast-cancer-survival-by-stage. [Last accessed on 2016 Jan 12].
- Hanrahan EO, Gonzalez-Angulo AM, Giordano SH, Rouzier R, Broglio KR, Hortobagyi GN, et al. Overall survival and cause-specific mortality of patients with stage T1a, bN0M0 breast carcinoma. J Clin Oncol 2007;25:4952-60.
- Herndon JE 2nd, Kornblith AB, Holland JC, Paskett ED. Effect of socioeconomic status as measured by education level on survival in breast cancer clinical trials. Psychooncology 2013;22:315-23.
- Hunter CP. Epidemiology, stage at diagnosis, and tumor biology of breast carcinoma in multiracial and multiethnic populations. Cancer 2000;88:1193-202.
- Memon ZA, Shaikh AN, Rizwan S, Sardar MB. Reasons for patient's delay in diagnosis of breast carcinoma in Pakistan. Asian Pac J Cancer Prev 2013;14:7409-14.
- Miller AB. Mammography: A critical evaluation of its role in breast cancer screening, especially in developing countries. J Public Health Policy 1989;10:486-98.
- Babu GR, Lakshmi SB, Thiyagarajan JA. Epidemiological correlates of breast cancer in south India. Asian Pac J Cancer Prev 2013;14:5077-83.
- MacKinnon JA, Duncan RC, Huang Y, Lee DJ, Fleming LE, Voti L, et al. Detecting an association between socioeconomic status and late stage breast cancer using spatial analysis and area-based measures. Cancer Epidemiol Biomarkers Prev 2007;16:756-62.
- Sharma K, Costas A, Shulman LN, Meara JG. A systematic review of barriers to breast cancer care in developing countries resulting in delayed patient presentation. J Oncol 2012;2012:121873.
- Harirchi I, Ghaemmaghami F, Karbakhsh M, Moghimi R, Mazaherie H. Patient delay in women presenting with advanced breast cancer: An Iranian study. Public Health 2005;119:885-91.
- Leong SP, Shen ZZ, Liu TJ, Agarwal G, Tajima T, Paik NS, et al. Is breast cancer the same disease in Asian and western countries? World J Surg 2010;34:2308-24.
- Gadgil A, Roy N, Sankaranarayanan R, Muwonge R, Sauvaget C. Effect of comprehensive breast care on breast cancer outcomes: A community hospital based study from Mumbai, India. Asian Pac J Cancer Prev 2012;13:1105-9.
- Miller BA, Hankey BF, Thomas TL. Impact of sociodemographic factors, hormone receptor status, and tumor grade on ethnic differences in tumor stage and size for breast cancer in US women. Am J Epidemiol 2002;155:534-45.
- Mohaghegh P, Yavari P, Akbari ME, Abadi A, Ahmadi F. Associations of demographic and socioeconomic factors with stage at diagnosis of breast cancer. Asian Pac J Cancer Prev 2015;16:1627-31.
- Richardson JL, Langholz B, Bernstein L, Burciaga C, Danley K, Ross RK, et al. Stage and delay in breast cancer diagnosis by race, socioeconomic status, age and year. Br J Cancer 1992;65:922-6.
- Satariano WA, Ragland DR. The effect of comorbidity on 3-year survival of women with primary breast cancer. Ann Intern Med 1994;120:104-10.
- Neal RD, Allgar VL. Sociodemographic factors and delays in the diagnosis of six cancers: Analysis of data from the “National survey of NHS patients: Cancer”. Br J Cancer 2005;92:1971-5.
- Meechan G, Collins J, Petrie K. Delay in seeking medical care for self-detected breast symptoms in New Zealand women. N Z Med J 2002;115:U257.
- Ramirez AJ, Westcombe AM, Burgess CC, Sutton S, Littlejohns P, Richards MA, et al. Factors predicting delayed presentation of symptomatic breast cancer: A systematic review. Lancet 1999;353:1127-31.
- Burgess CC, Ramirez AJ, Richards MA, Love SB. Who and what influences delayed presentation in breast cancer? Br J Cancer 1998;77:1343-8.
- Meechan G, Collins J, Petrie KJ. The relationship of symptoms and psychological factors to delay in seeking medical care for breast symptoms. Prev Med 2003;36:374-8.
- Yip CH, bt Mohd Taib NA, Lau PC. Does a positive family history influence the presentation of breast cancer? Asian Pac J Cancer Prev 2008;9:63-5.