 PDF
PDF  Views
Views  Share
Share


Relation of Serum Prostate-Specific Antigen with Histological Features and Grading of Prostate Adenocarcinoma in Prostatic Biopsies
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2020; 41(02): 193-197
DOI: DOI: 10.4103/ijmpo.ijmpo_25_18
Abstract
Introduction: The present study was undertaken on cases of prostate carcinoma and we tried to determine the relationship of elevated prostate specific antigen (PSA) level to histopathologic features associated with cancer in prostate biopsies and their relation to newest grade groups. Materials and Methods: The study was conducted in a tertiary health care center over a span of 3 years on patients with prostatic adenocarcinoma. The hematoxylin and eosin sections were reviewed as per World Health Organization 2016 new grading system and various other associated histopathological findings in the tissue noted. We tried to analyse correlation between serum PSA levels and histopathological features. Results: The majority of patients were in the age group of 70–80. Many patients (9/44) had the PSA in the range of 20–40 ng/ml and 10 patients (22.7%) had 80–100 ng/ml. There were three patients with normal PSA level and six patients with borderline level. Nine of 10 patients with marked increase in PSA level had higher grade groups. Histological subtyping showed 42 cases of acinar adenocarcinoma and 2 cases of ductal carcinoma. A number of associated findings were seen like benign prostatic hyperplasia (BPH): 13 cases, prostatitis: 28 cases, prostatic intraepithelial neoplasia: 7 cases - Low grade (1 case) and high grade (6 cases), and atrophy: 9 cases. Conclusions: We noticed majority of patients with grade group (GG) 3 and above had PSA value of more than 40 ng/ml, but PSA of <40 ng/ml did not correlate with the histologic grade groups. There was significant cut off value of PSA level 20 ng/ml between GG2 and GG3, differentiation of which is of clinical and histopathological significance. Histological subtyping showed acinar adenocarcinoma has no significant correlation with PSA levels however ductal carcinoma was associated with PSA levels <20 ng/ml. BPH association was seen to have PSA level of <40 ng/ml in majority of cases. The intensity of inflammation did not correlate with either degree of PSA level or histologic GG. We concluded serum PSA assay has prognostic application in the evaluation of patients undergoing prostate biopsies.
Keywords
Associated histological features - carcinoma prostate - Gleason’s grading - serum prostate-specific antigenPublication History
Received: 31 January 2018
Accepted: 12 November 2019
Article published online:
23 May 2021
© 2020. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Introduction: The present study was undertaken on cases of prostate carcinoma and we tried to determine the relationship of elevated prostate specific antigen (PSA) level to histopathologic features associated with cancer in prostate biopsies and their relation to newest grade groups. Materials and Methods: The study was conducted in a tertiary health care center over a span of 3 years on patients with prostatic adenocarcinoma. The hematoxylin and eosin sections were reviewed as per World Health Organization 2016 new grading system and various other associated histopathological findings in the tissue noted. We tried to analyse correlation between serum PSA levels and histopathological features. Results: The majority of patients were in the age group of 70–80. Many patients (9/44) had the PSA in the range of 20–40 ng/ml and 10 patients (22.7%) had 80–100 ng/ml. There were three patients with normal PSA level and six patients with borderline level. Nine of 10 patients with marked increase in PSA level had higher grade groups. Histological subtyping showed 42 cases of acinar adenocarcinoma and 2 cases of ductal carcinoma. A number of associated findings were seen like benign prostatic hyperplasia (BPH): 13 cases, prostatitis: 28 cases, prostatic intraepithelial neoplasia: 7 cases - Low grade (1 case) and high grade (6 cases), and atrophy: 9 cases. Conclusions: We noticed majority of patients with grade group (GG) 3 and above had PSA value of more than 40 ng/ml, but PSA of <40 ng/ml did not correlate with the histologic grade groups. There was significant cut off value of PSA level 20 ng/ml between GG2 and GG3, differentiation of which is of clinical and histopathological significance. Histological subtyping showed acinar adenocarcinoma has no significant correlation with PSA levels however ductal carcinoma was associated with PSA levels <20 ng/ml. BPH association was seen to have PSA level of <40 ng/ml in majority of cases. The intensity of inflammation did not correlate with either degree of PSA level or histologic GG. We concluded serum PSA assay has prognostic application in the evaluation of patients undergoing prostate biopsies.
Keywords
Associated histological features - carcinoma prostate - Gleason’s grading - serum prostate-specific antigenIntroduction
Prostate cancer is the most common cancer in men worldwide and is responsible for 20% of all newly diagnosed male cancers.[1] Serum prostate specific antigen (PSA) based screening is helpful in early diagnosis and staging of prostate cancer. PSA is the most important tumor marker which is used routinely and proved to have a positive correlation with tumor volume and pathological stage.[2] It is a protein produced by the cells of the prostate gland which is generally increased in diseases such as prostatitis, hyperplasia and malignancy but the correlation between various pathologies affecting the prostate gland and their corresponding rise in PSA values is not constant.[3] Recently, WHO has come out with latest modification of Gleason grading with categorization of prostate adenocarcinoma (PC) patients in 5 grade groups. We tried to determine the relationship of elevated PSA level in PC patients to histopathological features associated with cancer in prostate biopsies and their relation to newest grade groups.
Materials and Methods
This was a retrospective study carried out in the department of laboratory medicine, Aseer central hospital over a period of 3 years from January 2014 to December 2016. The clinical and laboratory data were collected from record section of the hospital, including the preoperative serum PSA level. PSA was measured by electrochemiluminescence immunoassay on Roche Elecsys immunoassay analyzer. The histopathology specimens included needle biopsies (33) and transurethral resection of prostate-11. The hematoxylin and eosin sections were reviewed for prostatic adenocarcinoma grading system as per WHO 2016 new grading system and various other associated histopathologic findings in the tissue noted.[4] We tried to analyze the correlation between serum PSA levels and histopathological features in terms of grading and other findings like inflammation, hyperplasia, atrophy and prostatic intraepithelial neoplasia (PIN). The patients were categorized according to PSA levels into groups – Group A: 0–4 ng/ml, B: 4.1–10 ng/ml, C: 10.1–20 ng/ml, D: 20.1–40 ng/ml, E: 40.1–60 ng/ml, F: 60.1–80 ng/ml, G: 80.1–100 ng/ml, H >100 ng/ml.
Results
A total of 100 prostatic cases were received, of which 56 were diagnosed as benign and 44 as PC.
The majority of patients of PC were in the age group of 70–80 (50%). Only 2 patients were <60 and 6 patients were above 80 years of age. The intensity of raised PSA does not appear to be proportional to increasing age as older patients are distributed randomly in the PSA range of 20–100 ng/ml [Chart 1].
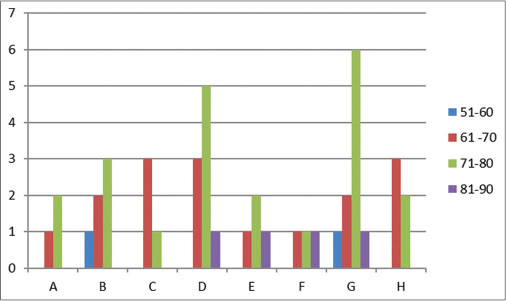
| Chart 1: Relation of prostate‑specific antigen level with age group of patients
Many patients (9/44) belong to the PSA range of 20–40 ng/ml and 10 patients (22.7%) belong to 80–100 ng/ml. There were three patients with normal PSA levels and 6 patients with borderline levels [Table 1].
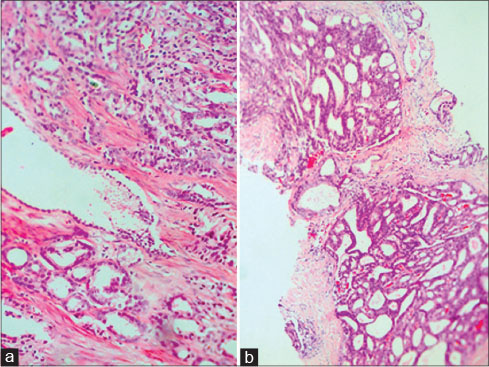
Gleason grading was done according to latest classification and grade group: GG1: 2 cases [Figure 1]a, GG2: 4 cases [Figure 1]b, GG3: 8 cases [Figure 2]a, GG4: 7 cases [Figure 2]b, and GG5: 23 cases [Figure 3]a and b] were noted. The maximum number of patients (10 of 44 cases) showed marked increase in PSA level (80–100 ng/ml) and 9 of them belonged to higher grade groups, though the higher grade groups of 4 or 5 are also noted in other PSA level groups. In GG1 patients, PSA levels varied from 4 to 20 ng/ml; in GG2 patients, PSA varied from 0 to 40 ng/ml; in GG3 patients, PSA range from 0 to 100 ng/ml; in GG4 patients, PSA was seen from 4 to above 100 ng/ml; in GG5 cases, PSA showed significant variation from 0 to above 100 ng/ml although in majority of GG5 patients (20 out of 23 cases), it was above 20 ng/ml. PSA value of above 40 ng/ml indicates higher grade groups of 3 and above, and PSA of <40 ng/ml does not correlate with histologic grade groups. Two cases of GG3 showed PSA of <10 whereas 6 GG3 cases showed a PSA value above 20 ng/ml. All cases of GG2 patients showed PSA of <40, but in 3 out of 4 cases PSA was <20 ng/ml.
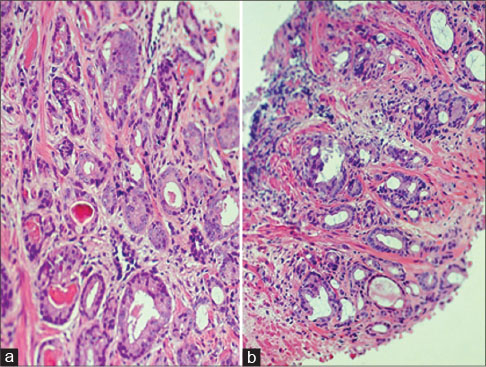
| Figure 1: (a and b) Sections showing malignant glands with cells exhibiting pleomorphism, vesicular nuclei and nucleoli with GG 1: Gleason score 6 and GG 2: Gleason score 3 + 4 = 7 respectively (H and E, a and b: ×20)
| Figure 2: (a and b) Sections showing malignant glands with cells exhibiting pleomorphism, vesicular nuclei and nucleoli with GG 3: Gleason score 4 + 3 = 7 and GG 4: Gleason score 8, respectively (H and E, a and b: ×20)
| Figure 3: (a and b) Sections showing GG 5: Gleason score 4 + 5 = 9 and 10, respectively (H and E, a: ×40, b: ×20)
Histological typing
Majority of cases were acinar adenocarcinoma: 42 cases (95.6%) followed by invasive ductal carcinoma: 2 cases (4.5% ). 13 cases of PC had PSA levels below 20 ng/ml, of which 9 were acinar adenocarcinoma and 2 were invasive ductal carcinoma [Table 2].
|
PSA (ng/ml) |
Histological typing of carcinomas |
GGs |
|---|---|---|
|
GGs – Grade group; PSA – Prostate-specific antigen |
||
|
0.3 |
Acinar adenocarcinoma |
2 |
|
2.31 |
Acinar adenocarcinoma with predominant single |
5 |
|
cell pattern |
||
|
2.76 |
Acinar adenocarcinoma |
3 |
|
4.29 |
Acinar adenocarcinoma |
2 |
|
4.88 |
Invasive ductal carcinoma with urothelial |
4 |
|
differentiation |
||
|
5.05 |
Acinar adenocarcinoma on hormonal treatment |
5 |
|
7.8 |
Acinar adenocarcinoma |
3 |
|
8.05 |
Pseudohyperplastic variant of acinar adenocarcinoma |
1 |
|
9.22 |
Acinar adenocarcinoma |
5 |
|
11.49 |
Foamy cell variant of acinar adenocarcinoma |
2 |
|
13.03 |
Acinar adenocarcinoma |
4 |
|
15.6 |
Acinar adenocarcinoma |
1 |
|
16.17 |
Invasive ductal carcinoma |
4 |
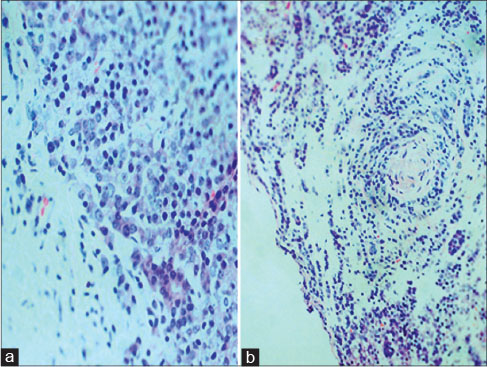
A number of associated findings were seen like prostatitis: 28 cases [Figure 4]a, benign prostatic hyperplasia (BPH): 13 cases [Figure 4]b, atrophy: 9 cases [Figure 5]a, PIN: 7 cases - Low grade: 1 case and high grade: 6 cases [Figure 5]b. Among associated BPH patients, majority of them (11 of 13 cases) showed PSA of <40 ng/ml. Nineteen patients with associated prostatitis showed elevated PSA ranging from 10 ng/ml to 100 ng/ml and six patients between 4 and 10 ng/ml. In majority of the patients (26 of 28 cases), the inflammation was mild to moderate. The intensity of PSA rise was not correlating with intensity of inflammation. PSA level ranged from 4 to 100 in cases associated with PIN irrespective of low or high grade PIN, but in cases of retrograde PIN and micropapillary type of PIN, it was above 20 ng/ml. Large number of atrophy associated cases (7 of 9 cases), PSA level varied from 10 to 80 ng/ml, of which 3 cases of inflammatory atrophy showed PSA value of 60–100 ng/ml.
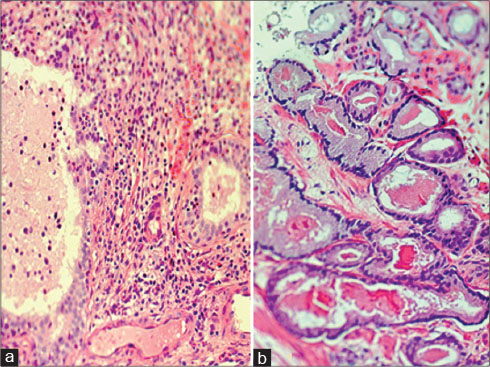
| Figure 4: (a) Section showing inflammatory cells and glands of prostate and (b) section showing hyperplasia in prostatic glands (H and E, a and b: ×20)
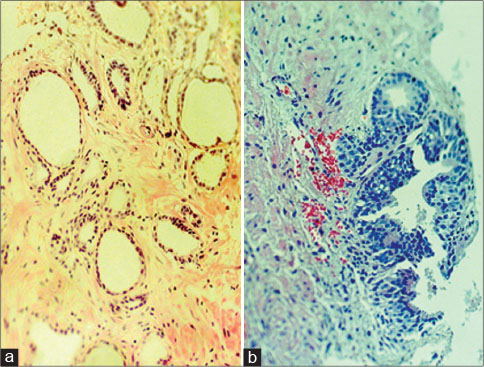
| Figure 5: (a) Section showing atrophic glands and (b) section showing HGPIN (H and E, a and b: ×20)
Discussion
PSA is a glycoprotein, a kallikrein-like protease produced by the epithelial cells which line the ducts and acini of prostate gland.[5] Serum PSA assay has been widely used as a screening test for PC, though it is known to be elevated in various benign conditions of prostate, post digital rectal examination and instrumentation. All our patients were above 50 years of age with majority (50%) between 70 to 80 years. This goes well with another study where peak age incidence of PC was 7th decade.[6] The intensity of raised PSA does not appear to be proportional to increasing age as older patients are distributed randomly in the PSA range of 20 to 100 ng/ml.
Abu Farsakh andAbu Farsakh found 11% of PC patients with normal serum PSA whereas 6.8% of our patients belonged to this group.[7] The patients with PSA values between 0 and 4 ng/ml: 6.8%; 4–10 ng/ml: 13.6%; 10–20 ng/ml: 9%, and above 20 ng/ml: 70.4% were comparable with another study of Jose et al., where these were 3.6%, 13.3%, 16.6% and 66.5% respectively,[6] indicating around 80% patients show elevated PSA above 10 ng/ml.
The histopathological Gleason grading system is a very significant prognostic factor used in risk stratification of PC patients while deciding management.[8] A new set of grade groups was recently developed at the 2014 International Society of Urological Pathology consensus conference on Gleason grading of PC which was accepted and published by WHO in 2016. These grade groups are as follows: GG 1: Gleason score (GS) 6, GG 2: GS 3 + 4 = 7, GG 3: GS 4 + 3 = 7, GG 4: GS 4 + 4 = 8, 3 + 5 = 8, 5 + 3 = 8, GG 5: GS 9–10. GS 6 is the lowest possible grade rather than an intermediate grade 6 of 10 and carries an excellent prognosis.[9] [10]
Majority (23/44) of our patients were in GG5. In GG5 cases, PSA showed a significant variation from 0 to above 100 ng/ml though in majority of GG5 patients (20 out of 23 cases), it was above 20 ng/ml. PSA levels ranged from 4 to 20 ng/ml in GG1 which was observed in only two patients. A PSA value of above 40 ng/ml indicates higher GGs of 3 and above but PSA of <40 ng/ml does not correlate with histologic grade groups. Abu Farsakh andAbu Farsakh, observed no definite relationship between PSA and GS,[7] but we found similar results in cases with PSA value of <40 ng/ml. However, in cases of PSA above 40, an elevated serum PSA level is more likely to be correlating with higher grade of carcinoma, similar to study of Jose et al.[6] We also noticed an interesting correlation of PSA level with GG2 and GG3, as majority of GG3 patients showed values above 20 and majority of GG2 patients were below 20.
PC can be divided into two major histologic categories: acinar and ductal. Unusual histological variants of PC include atrophic carcinoma, pseudo hyperplastic carcinoma, foamy gland carcinoma, mucinous (colloid) carcinoma, signet ring cell carcinoma, basal cell and adenoid cystic carcinoma, squamous cell carcinoma, PC with neuroendocrine differentiation and sarcomatoid carcinoma, aberrant p63 expressing carcinoma.[5] PSA level <20 ng/ml included 6 cases of high grade (GG 4 and 5) of which 4 were acinar adenocarcinoma and 2 were ductal type. Acinar types had PSA levels ranging between 0 and >100 ng/ml however the 2 cases of ductal carcinomas had PSA <20 ng/ml. Patients with ductal carcinomas present with lower PSA, have more favorable pathological features, and similar overall survival compared to men with Gleason 8–10 acinar adenocarcinoma.[11]
Bostwick et al., found most cancers in prostates with concomitant BPH (83.3%).[12] However, in our study, only 13 cases (29.5%) had features of BPH. This may be due to type of sampling, in current study, majority are of core needle biopsies. Yeboah and Hsing, are of the opinion that association with BPH may be due to associated inflammation or hormonal milieu changes being conducive for malignant growth and they doubt BPH as a cofactor for PC risk.[13] Among associated BPH patients, majority of them (11 of 13 cases) showed PSA of <40 ng/ml. BPH and PC are part of the metabolic syndrome with inflammation emerging as a major contributor to the development of both.[14] In majority of our patients (26 of 28 cases), the inflammation was mild to moderate. The degree of PSA rise was not correlating with intensity of inflammation. Histological specimens of prostate cancer tissue frequently exhibit unexplained acute and chronic inflammation and inflammation associated lesions.[15]
It has been claimed that PIN does not result in elevated PSA levels and low-grade PIN is a relatively common finding in young male patients.[16] Present study showed PSA level ranged from 4 to 100 in cases associated with PIN irrespective of low or high grade PIN, but in cases of retrograde PIN and micropapillary type of PIN, it was above 20 ng/ml. This likely explains that the associated invasive carcinoma, rather than the PIN itself gives rise to high PSA levels, which in turn may postulate the associated new mutation in invasive cancer. In the study by Haffner et al., lesions meeting morphologic criteria for high-grade PIN that were adjacent to carcinoma may represent invasive carcinoma colonizing benign glands in a retrograde manner so that not all lesions regarded as PIN represent precursors.[17]
In large number of atrophy associated cases (7 of 9 cases) PSA level varied from 10 to 80 ng/ml, of which 3 cases of inflammatory atrophy showed PSA value of 60–100 ng/ml. There was a positive and significant association between extent of atrophy and PSA elevation. The authors hypothesize that injurious stimuli causing focal prostatic atrophy may interfere in the physiologic barrier that prevents the escape of any significant amounts of PSA to the general circulation.[18] Proliferative inflammatory atrophy (PIA) which is recognized as a direct precursor to many PC like high-grade PIN, have some of the hallmark somatic genome alterations found in PC. Instances of PIA directly merging with cancer were identified in 28% of the cases.[19] Current study showed very high PSA level in cases of PC associated with PIA, though the cases were only 3 out of 44; which may suggest PIA as an associated high risk precursor lesion.
Conclusions
We tried to correlate serum PSA level with the age of the patient, latest grade groups of carcinoma and other associated histological features. Most of the patients belonged to 70–80 years age group but PSA levels did not appear to be proportional to increasing age. Majority of patients with GG3 and above showed PSA value of more than 40 ng/ml but PSA of <40 did not correlate with the histologic grade groups. There was significant cutoff value of PSA level of 20 ng/ml, between GG2 and GG3, differentiation of which is of clinical and histopathological significance. Ductal adenocarcinoma was associated with low levels of PSA. BPH association was seen to have PSA level of <40 ng/ml in majority of cases. Though 28 of 44 cases showed associated inflammation but the intensity did not correlate with either degree of PSA level or histologic GG. The higher PSA level appears to have direct correlation with retrograde PIN and PIA. We found serum PSA assay has prognostic application in the evaluation of patients undergoing prostate biopsies with proper interpretation. We also recommend further genomic study for correlation with serum PSA level in various possibly related histopathological prostate lesions.
Conflict of Interest
There are no conflicts of interest.
References
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin 2016; 66: 7-30
- Andriole GL, Crawford ED, Grubb 3rd RL, Buys SS, Chia D, Church TR. et al. Prostate cancer screening in the randomized prostate, lung, colorectal, and ovarian cancer screening trial: mortality results after 13 years of follow-up. J Natl Cancer Inst 2012; 104: 125-32
- Schröder FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S, Nelen V. et al. Prostate-cancer mortality at 11 years of follow-up. N Engl J Med 2012; 366: 981-90
- Moch H, Humphrey PA, Ulbright TM, Reuter V. WHO Classification of Tumours of the Urinary System and Male Genital Organs. Lyon, France: International Agency for Research on Cancer; 2016
- Rosai J, Ackerman L. Surgical Pathology. 11th ed. New York: Mosby; 2017
- Jose L, Suma MT, Sadasivan S, Souda VM. Gleason’s grading of carcinoma prostate with PSA correlation. J Med Sc Clin Res 2017; 5: 27634-9
- Abu Farsakh MG, Abu Farsakh HA. Serum prostate-specific antigen, radiologic findings and Gleason score in prostate biopsies in Jordan. Hematol Oncol Stem Cell Ther 2008; 1: 171-4
- Thompson I, Thrasher JB, Aus G, Burnett AL, Canby-Hagino ED, Cookson MS. et al. Guideline for the management of clinically localized prostate cancer: 2007 update. J Urol 2007; 177: 2106-31
- Epstein JI, Egevad L, Amin MB, Delahunt B, Srigley JR, Humphrey PA. et al. The 2014 International Society of Urological Pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma: Definition of grading patterns and proposal for a new grading system. Am J Surg Pathol 2016; 40: 244-52
- Epstein JI, Zelefsky MJ, Sjoberg DD, Nelson JB, Egevad L, Magi-Galluzzi C. et al. A contemporary prostate cancer grading system: A validated alternative to the Gleason score. Eur Urol 2016; 69: 428-35
- Packiam VT, Patel SG, Pariser JJ, Richards KA, Weiner AB, Paner GP. et al. Contemporary population-based comparison of localized ductal adenocarcinoma and high-risk Acinar adenocarcinoma of the prostate. Urology 2015; 86: 777-82
- Bostwick DG, Cooner WH, Denis L, Jones GW, Scardino PT, Murphy GP. The association of benign prostatic hyperplasia and cancer of the prostate. Cancer 1992; 70: 291-301
- Yeboah ED, Hsing AW. Benign prostatic hyperplasia and prostate cancer in Africans and Africans in the diaspora. J West Afr Coll Surg 2016; 6: x-xviii
- Alcaraz A, Hammerer P, Tubaro A, Schröder FH, Castro R. Editorial comment on: Is there evidence of a relationship between benign prostatic hyperpl Asia and prostate cancer? Findings of a literature review. Eur Urol 2009; 55: 873-4
- Sfanos KS, De Marzo AM. Prostate cancer and inflammation: The evidence. Histopathology 2012; 60: 199-215
- Ronnett BM, Carmichael MJ, Carter HB, Epstein JI. Does high grade prostatic intraepithelial neoplasia result in elevated serum prostate specific antigen levels?. J Urol 1993; 150: 386-9
- Haffner MC, Weier C, Xu MM, Vaghasia A, Gürel B, Gümüşkaya B. et al. Molecular evidence that invasive adenocarcinoma can mimic prostatic intraepithelial neoplasia (PIN) and intraductal carcinoma through retrograde glandular colonization. J Pathol 2016; 238: 31-41
- Billis A, Meirelles LR, Magna LA, Baracat J, Prando A, Ferreira U. Extent of prostatic atrophy in needle biopsies and serum PSA levels: Is there an association?. Urology 2007; 69: 927-30
- De Marzo AM, Platz EA, Sutcliffe S, Xu J, Grönberg H, Drake CG. et al. Inflammation in prostate carcinogenesis. Nat Rev Cancer 2007; 7: 256-69
Address for correspondence
Publication History
Received: 31 January 2018
Accepted: 12 November 2019
Article published online:
23 May 2021
© 2020. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
| Chart 1: Relation of prostate‑specific antigen level with age group of patients
| Figure 1: (a and b) Sections showing malignant glands with cells exhibiting pleomorphism, vesicular nuclei and nucleoli with GG 1: Gleason score 6 and GG 2: Gleason score 3 + 4 = 7 respectively (H and E, a and b: ×20)
| Figure 2: (a and b) Sections showing malignant glands with cells exhibiting pleomorphism, vesicular nuclei and nucleoli with GG 3: Gleason score 4 + 3 = 7 and GG 4: Gleason score 8, respectively (H and E, a and b: ×20)
| Figure 3: (a and b) Sections showing GG 5: Gleason score 4 + 5 = 9 and 10, respectively (H and E, a: ×40, b: ×20)
| Figure 4: (a) Section showing inflammatory cells and glands of prostate and (b) section showing hyperplasia in prostatic glands (H and E, a and b: ×20)
| Figure 5: (a) Section showing atrophic glands and (b) section showing HGPIN (H and E, a and b: ×20)
- 1 Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin 2016; 66: 7-30
- 2 Andriole GL, Crawford ED, Grubb 3rd RL, Buys SS, Chia D, Church TR. et al. Prostate cancer screening in the randomized prostate, lung, colorectal, and ovarian cancer screening trial: mortality results after 13 years of follow-up. J Natl Cancer Inst 2012; 104: 125-32
- 3 Schröder FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S, Nelen V. et al. Prostate-cancer mortality at 11 years of follow-up. N Engl J Med 2012; 366: 981-90
- 4 Moch H, Humphrey PA, Ulbright TM, Reuter V. WHO Classification of Tumours of the Urinary System and Male Genital Organs. Lyon, France: International Agency for Research on Cancer; 2016
- 5 Rosai J, Ackerman L. Surgical Pathology. 11th ed. New York: Mosby; 2017
- 6 Jose L, Suma MT, Sadasivan S, Souda VM. Gleason’s grading of carcinoma prostate with PSA correlation. J Med Sc Clin Res 2017; 5: 27634-9
- 7 Abu Farsakh MG, Abu Farsakh HA. Serum prostate-specific antigen, radiologic findings and Gleason score in prostate biopsies in Jordan. Hematol Oncol Stem Cell Ther 2008; 1: 171-4
- 8 Thompson I, Thrasher JB, Aus G, Burnett AL, Canby-Hagino ED, Cookson MS. et al. Guideline for the management of clinically localized prostate cancer: 2007 update. J Urol 2007; 177: 2106-31
- 9 Epstein JI, Egevad L, Amin MB, Delahunt B, Srigley JR, Humphrey PA. et al. The 2014 International Society of Urological Pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma: Definition of grading patterns and proposal for a new grading system. Am J Surg Pathol 2016; 40: 244-52
- 10 Epstein JI, Zelefsky MJ, Sjoberg DD, Nelson JB, Egevad L, Magi-Galluzzi C. et al. A contemporary prostate cancer grading system: A validated alternative to the Gleason score. Eur Urol 2016; 69: 428-35
- 11 Packiam VT, Patel SG, Pariser JJ, Richards KA, Weiner AB, Paner GP. et al. Contemporary population-based comparison of localized ductal adenocarcinoma and high-risk Acinar adenocarcinoma of the prostate. Urology 2015; 86: 777-82
- 12 Bostwick DG, Cooner WH, Denis L, Jones GW, Scardino PT, Murphy GP. The association of benign prostatic hyperplasia and cancer of the prostate. Cancer 1992; 70: 291-301
- 13 Yeboah ED, Hsing AW. Benign prostatic hyperplasia and prostate cancer in Africans and Africans in the diaspora. J West Afr Coll Surg 2016; 6: x-xviii
- 14 Alcaraz A, Hammerer P, Tubaro A, Schröder FH, Castro R. Editorial comment on: Is there evidence of a relationship between benign prostatic hyperpl Asia and prostate cancer? Findings of a literature review. Eur Urol 2009; 55: 873-4
- 15 Sfanos KS, De Marzo AM. Prostate cancer and inflammation: The evidence. Histopathology 2012; 60: 199-215
- 16 Ronnett BM, Carmichael MJ, Carter HB, Epstein JI. Does high grade prostatic intraepithelial neoplasia result in elevated serum prostate specific antigen levels?. J Urol 1993; 150: 386-9
- 17 Haffner MC, Weier C, Xu MM, Vaghasia A, Gürel B, Gümüşkaya B. et al. Molecular evidence that invasive adenocarcinoma can mimic prostatic intraepithelial neoplasia (PIN) and intraductal carcinoma through retrograde glandular colonization. J Pathol 2016; 238: 31-41
- 18 Billis A, Meirelles LR, Magna LA, Baracat J, Prando A, Ferreira U. Extent of prostatic atrophy in needle biopsies and serum PSA levels: Is there an association?. Urology 2007; 69: 927-30
- 19 De Marzo AM, Platz EA, Sutcliffe S, Xu J, Grönberg H, Drake CG. et al. Inflammation in prostate carcinogenesis. Nat Rev Cancer 2007; 7: 256-69