 PDF
PDF  Views
Views  Share
Share


Primary Leiomyosarcoma of Breast Presenting with Metastasis: An Atypical Presentation with Dismal Prognosis
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(04): 535-537
DOI: DOI: 10.4103/ijmpo.ijmpo_139_16
Abstract
Leiomyosarcoma is an extremely uncommon subtype of breast sarcoma, with <-50-cases reported in the English literature till date. Patients usually present at an early stage and follow an indolent course. We reported an unusual case of leiomyosarcoma of breast in a post -menopausal female,presented with right side breast lump and pain right side hip. Histomorphological evaluation and immunohistochemistry confirmed the diagnosis. The patient received palliative radiotherapy 20 Gy in 5 fractions to right iliac bone and was started on chemotherapycomprising of docetaxel and epirubicin. Leiomyosarcoma of breast is known to have local recurrence and hematogenous metastasis, usually 10–15 years after the primary diagnosis. Aggressive behavior of leiomyosarcomas in the form of such a rapidly growing, fungating mass of 15 cm in greatest dimension with hematogenous metastasis at the time of initial presentation, as seen in our case, is extremely unusual.
Publication History
Article published online:
04 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used forcommercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Leiomyosarcoma is an extremely uncommon subtype of breast sarcoma, with <-50-cases reported in the English literature till date. Patients usually present at an early stage and follow an indolent course. We reported an unusual case of leiomyosarcoma of breast in a post -menopausal female,presented with right side breast lump and pain right side hip. Histomorphological evaluation and immunohistochemistry confirmed the diagnosis. The patient received palliative radiotherapy 20 Gy in 5 fractions to right iliac bone and was started on chemotherapycomprising of docetaxel and epirubicin. Leiomyosarcoma of breast is known to have local recurrence and hematogenous metastasis, usually 10–15 years after the primary diagnosis. Aggressive behavior of leiomyosarcomas in the form of such a rapidly growing, fungating mass of 15 cm in greatest dimension with hematogenous metastasis at the time of initial presentation, as seen in our case, is extremely unusual.
Introduction
Primary breast sarcomas are rare neoplasms, with a reported incidence of 1% of breast tumors.[1] Among these, leiomyosarcoma is an extremely uncommon subtype, with <50 xss=removed>cases reported till date. These tumors usually present at an early stage and follow an indolent course. Scattered case reports of nodal metastasis are on record; however, aggressive clinical behavior and distant metastasis are rarely reported, if at all after 10–15 years of primary diagnosis. Owing to the paucity of literature, the prognostic factors which can predict the biological behavior in breast leiomyosarcomas have not been reported yet.
We reported such an atypical case of primary breast leiomyosarcoma in a postmenopausal female along with a brief review of the literature. Our case is unusual in view of the large and rapidly growing tumor mass, lymph nodes, and bone metastasis at the time of presentation, denoting its aggressive behavior and poor prognosis.
Case Report
A 48 year postmenopausal female presented to surgery outpatient department with a lump in the right breast. She noticed the lump for the past one and a half years, which progressively increased in size and ulcerated the overlying skin. She also gave a history of pain in the right hip region for the last one week. There was no family history of breast or ovarian cancer. Local examination revealed a hard, fungating, lump in the right breast measuring 16 cm × 10 cm and involving all the four quadrants. The overlying skin along with nipple–areola complex was ulcerated. The lump was immobile and fixed to the underlying chest wall muscles. Contralateral breast was unremarkable. Further examination revealed limited and painful right hip joint movement along with tenderness. Routine laboratory investigations were within normal limits. Positron emission tomography scan showed a large lobular mass in the right breast measuring 15.3 cm × 12.5 cm × 9 cm showing intense metabolic uptake (SUV 17.5), with the left axillary lymph node measuring 1.2 cm × 0.9 cm (SUV 2) and with the right axillary lymph nodes measuring 1.2 cm × 0.9 cm (SUV 2) along with the right lung lesion and lytic lesion in the right iliac bone [Figure 1]. With a clinico-radiological diagnosis of breast carcinoma with the lymph nodes and bone metastases, stage cT4bN0M1 was assigned, and core needle biopsy was performed. Microscopic features were suggestive of a high-grade spindle cell neoplasm. The case was discussed in the multidisciplinary clinic and planned for palliative treatment. The patient received palliative chemotherapy followed by toilet mastectomy. The mastectomy specimen was fixed in 10% neutral buffered formalin and sent for histopathological examination. Gross examination revealed a modified radical mastectomy specimen with an ulcerated nipple–areola complex [Figure 2a]. On serial sections, a fungating, hard tumor (15.5 cm × 13.5 cm × 9 cm) was seen involving all the quadrants. Cut surface revealed a gray-white and fleshy tumor with areas of hemorrhage and necrosis [Figure 2b]. Microscopic examination revealed an infiltrative tumor comprising of spindle to elongated cells arranged in intersecting fascicles and bundles [Figure 3a]. Individual tumor cells had moderate amount of eosinophilic cytoplasm, oval to elongated cigar-shaped nuclei, vesicular chromatin, and single conspicuous nucleolus [Figure 3b]. A fair number of atypical mitoses were seen [Figure 3c]. On immunohistochemistry, these tumor cells were positive for vimentin and smooth muscle actin (SMA) [Figure 3d] and negative for desmin, pan cytokeratin (panCK), epithelial membrane antigen (EMA), S100, and neuron-specific enolase. Based on the immunomorphological features, a final diagnosis of leiomyosarcoma of the right breast was rendered. The patient received palliative radiotherapy 20 Gy in 5 fractions to the right iliac bone and was started on chemotherapy comprising of docetaxel and epirubicin with injection Zoledronic acid 4 mg monthly. Good palliation was achieved after radiotherapy and chemotherapy.
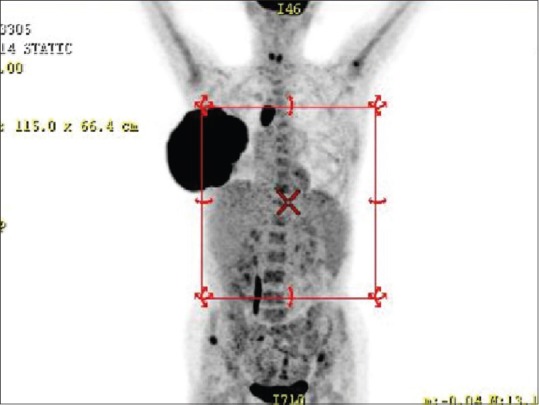
| Figure 1:Positron emission tomography scan shows a large lobulated mass in the right breast showing intense metabolic uptake (SUV 17.5), with the left axillary lymph node measuring 1.2 cm × 0.9 cm (SUV 2) with lung and bone metastasis

| Figure 2:(a) Gross photograph of a mastectomy specimen shows a gray-white, hard, circumscribed, and fungating tumor measuring 15.5 cm × 13.5 cm × 9 cm. There is ulceration of the overlying skin and nipple–areola complex (b) Cut surface of tumor is gray-white and fleshy
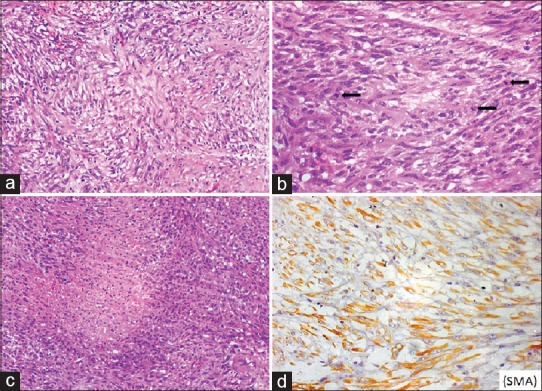
| Figure 3:Photomicrograph showing (a) a poorly circumscribed tumor comprising of the spindle-to-elongated cells arranged in intersecting fascicles and bundles (H and E; ×200) (b) Individual tumor cells have moderate amount of eosinophilic cytoplasm, oval-to-elongated nuclei, vesicular chromatin, and conspicuous nucleolus. Numerous atypical mitoses are noted shown by arrows (H and E; ×400) (c) Areas of necrosis were seen (H and E; ×200) (d) On immunohistochemistry, these tumor cells show cytoplasmic positivity for S
Discussion
Primary leiomyosarcoma of the breast is an extremely rare tumor with an indolent clinical course. Regarding origin, it has been postulated that the tumor might arise from the smooth muscle of the lactiferous ducts of the nipple–areola complex and the surrounding blood vessels. Breast sarcoma usually presents as a large circumscribed slow-growing localized mass, with a median age of presentation being 56 years.[2] Our patient presented with a large, rapidly growing, fungating, and infiltrative tumor measuring 15.5 cm × 13.5 cm × 9 cm, which is the largest breast leiomyosarcoma of the documented cases. The behavior of leiomyosarcoma is unpredictable. The lymphatic route of spread is uncommon, with palpable lymphadenopathy seen in <10 href="https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5759077/#ref3" rid="ref3" class=" bibr popnode tag_hotlink tag_tooltip" id="__tag_659253979" role="button" aria-expanded="false" aria-haspopup="true" xss=removed>3] Thus, axillary dissection is believed to be unnecessary in such cases. However, distant hematogenous metastasis to the lungs, liver, and bone has been documented in approximately 25%-cases, which was seen after a latent period of 15–20 years. Chen et al. reported a similar case who presented with liver metastasis 16 years after simple mastectomy.[4]
Our patient presented with both axillary and mediastinal lymphadenopathy and distant hematogenous metastasis. Borrowing from literature, most of the reported cases had presented at an early stage with a localized breast lump; in contrast, ours is the first case of breast leiomyosarcoma with bone metastasis at the time of initial presentation.
Simple mastectomy or lumpectomy followed by palliative chemotherapy/radiotherapy remains the mainstay of treatment. Histopathology along with immunohistochemistry is confirmatory and helpful in differentiation from other sarcomas, spindle cell myoepithelioma, and metaplastic carcinoma, which is imperative for patient management and prognosis.[5,6] Immunoreactivity for SMA and vimentin, and negative immunostaining for panCK and EMA exclude the possibility of metaplastic carcinoma.
Conclusion
Primary leiomyosarcoma is an uncommon indolent breast tumor known to have local recurrence and hematogenous metastasis usually after a period of 10–15 years. Albeit rare, such a large, rapidly growing tumor presenting with metastases signifies an aggressive behavior of breast leiomyosarcoma. Clinicians and pathologists must be aware of the same. Furthermore, hematogenous and nodal metastasis at the time of initial presentation makes this case unusual and interesting, emphasizing the need for careful lymph node evaluation in breast sarcomas. There are only few cases reported in the English literature with systemic spread and aggressive behavior, so there is a need for further studies to determine the prognostic factors which can predict the aggressive biological behavior in breast leiomyosarcomas. Hence poor prognostic factors are yet to be discovered.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Adem C, Reynolds C, Ingle JN, Nascimento AG. Primary breast sarcoma: Clinicopathologic series from the Mayo clinic and review of the literature. Br J Cancer 2004;91:237-41.
- Hussien M, Sivananthan S, Anderson N, Shiels A, Tracey N, Odling-Smee GW, et al. Primary leiomyosarcoma of the breast: Diagnosis, management and outcome. A report of a new case and review of literature. Breast 2001;10:530-4.
- Gullett NP, Delman K, Folpe AL, Johnstone PA. National surgical patterns of care: Regional lymphadenectomy of breast sarcomas. Am J Clin Oncol 2007;30:461-5.
- Chen KT, Kuo TT, Hoffmann KD. Leiomyosarcoma of the breast: A case of long survival and late hepatic metastasis. Cancer 1981;47:1883-6.
- Arista-Nasr J, Gonzalez-Gomez I, Angeles-Angeles A, Illanes-Baz E, Brandt-Brandt H, Larriva-Sahd J, et al. Primary recurrent leiomyosarcoma of the breast. Case report with ultrastructural and immunohistochemical study and review of the literature. Am J Clin Pathol 1989;92:500-5.
- Lawrence W Jr., Donegan WL, Natarajan N, Mettlin C, Beart R, Winchester D, et al. Adult soft tissue sarcomas. A pattern of care survey of the American College of Surgeons. Ann Surg 1987;205:349-59.
| Figure 1:Positron emission tomography scan shows a large lobulated mass in the right breast showing intense metabolic uptake (SUV 17.5), with the left axillary lymph node measuring 1.2 cm × 0.9 cm (SUV 2) with lung and bone metastasis
| Figure 2:(a) Gross photograph of a mastectomy specimen shows a gray-white, hard, circumscribed, and fungating tumor measuring 15.5 cm × 13.5 cm × 9 cm. There is ulceration of the overlying skin and nipple–areola complex (b) Cut surface of tumor is gray-white and fleshy
| Figure 3:Photomicrograph showing (a) a poorly circumscribed tumor comprising of the spindle-to-elongated cells arranged in intersecting fascicles and bundles (H and E; ×200) (b) Individual tumor cells have moderate amount of eosinophilic cytoplasm, oval-to-elongated nuclei, vesicular chromatin, and conspicuous nucleolus. Numerous atypical mitoses are noted shown by arrows (H and E; ×400) (c) Areas of necrosis were seen (H and E; ×200) (d) On immunohistochemistry, these tumor cells show cytoplasmic positivity for S
References
- Adem C, Reynolds C, Ingle JN, Nascimento AG. Primary breast sarcoma: Clinicopathologic series from the Mayo clinic and review of the literature. Br J Cancer 2004;91:237-41.
- Hussien M, Sivananthan S, Anderson N, Shiels A, Tracey N, Odling-Smee GW, et al. Primary leiomyosarcoma of the breast: Diagnosis, management and outcome. A report of a new case and review of literature. Breast 2001;10:530-4.
- Gullett NP, Delman K, Folpe AL, Johnstone PA. National surgical patterns of care: Regional lymphadenectomy of breast sarcomas. Am J Clin Oncol 2007;30:461-5.
- Chen KT, Kuo TT, Hoffmann KD. Leiomyosarcoma of the breast: A case of long survival and late hepatic metastasis. Cancer 1981;47:1883-6.
- Arista-Nasr J, Gonzalez-Gomez I, Angeles-Angeles A, Illanes-Baz E, Brandt-Brandt H, Larriva-Sahd J, et al. Primary recurrent leiomyosarcoma of the breast. Case report with ultrastructural and immunohistochemical study and review of the literature. Am J Clin Pathol 1989;92:500-5.
- Lawrence W Jr., Donegan WL, Natarajan N, Mettlin C, Beart R, Winchester D, et al. Adult soft tissue sarcomas. A pattern of care survey of the American College of Surgeons. Ann Surg 1987;205:349-59.