 PDF
PDF  Views
Views  Share
Share


Pretherapeutic Assessment by Multidetector Computed Tomography for Thyroid Cartilage Invasion in Laryngeal Cancer: A Double?edged Sword
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2018; 39(02): 196-202
DOI: DOI: 10.4103/ijmpo.ijmpo_101_17
Abstract
Introduction:Almost one-fourth of head and neck cancers in India are laryngeal cancers. Both conservative and surgical therapeutic approaches are available. According to present tumor-node-metastasis staging protocol, thyroid cartilage invasion is a crucial criterion for diagnosing advanced stages of the disease. A major cartilage invasion depicts T4A stage of disease for which surgical treatment is required. Aims: The present study aims to evaluate the accuracy of multidetector computed tomography (MDCT) in evaluation thyroid cartilage invasion in T3 and T4 stage of laryngeal cancers. Materials and Methods: It is a retrospective analysis done in the Department of Radiology, Pramukhswami Medical College, Anand, Gujarat, on 22 patients of T3 and T4 stage of laryngeal cancer who presented for pretherapeutic MDCT neck evaluation. The MDCT results were retrospectively reviewed and compared with postoperative histopathological results. Statistical analysis was done for each parameter as positive predictive value (PPV) (main statistical parameter), negative predictive value, sensitivity, and specificity. Results: MDCT showed a PPV of 60.00% in detecting any type of thyroid cartilage invasion, 66.66% for major and 33.33% for minor cartilage invasion. Extralaryngeal spread of disease was the most specific marker for cartilage involvement. In total, 31.8% of cases were downgraded in staging by pathology. Conclusion: Overestimation of thyroid cartilage invasion by MDCT is a reality which should be in mind before making final therapeutic decisions. Although crucial, it should not be the sole criteria preventing while making a surgical versus conservative therapeutic call.
Publication History
Article published online:
23 June 2021
© 2018. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Introduction:Almost one-fourth of head and neck cancers in India are laryngeal cancers. Both conservative and surgical therapeutic approaches are available. According to present tumor-node-metastasis staging protocol, thyroid cartilage invasion is a crucial criterion for diagnosing advanced stages of the disease. A major cartilage invasion depicts T4A stage of disease for which surgical treatment is required. Aims: The present study aims to evaluate the accuracy of multidetector computed tomography (MDCT) in evaluation thyroid cartilage invasion in T3 and T4 stage of laryngeal cancers. Materials and Methods: It is a retrospective analysis done in the Department of Radiology, Pramukhswami Medical College, Anand, Gujarat, on 22 patients of T3 and T4 stage of laryngeal cancer who presented for pretherapeutic MDCT neck evaluation. The MDCT results were retrospectively reviewed and compared with postoperative histopathological results. Statistical analysis was done for each parameter as positive predictive value (PPV) (main statistical parameter), negative predictive value, sensitivity, and specificity. Results: MDCT showed a PPV of 60.00% in detecting any type of thyroid cartilage invasion, 66.66% for major and 33.33% for minor cartilage invasion. Extralaryngeal spread of disease was the most specific marker for cartilage involvement. In total, 31.8% of cases were downgraded in staging by pathology. Conclusion: Overestimation of thyroid cartilage invasion by MDCT is a reality which should be in mind before making final therapeutic decisions. Although crucial, it should not be the sole criteria preventing while making a surgical versus conservative therapeutic call.
Introduction
Laryngeal cancer forms 1% of all diagnosed cancers. In India, its incidence varies from 1.26 to 8.18 per 1,00,000 individuals varying in different demographic distributions. Men are invariably more affected than women, and it is the seventh most common cause of cancer in Indian men.[1]
The association of laryngeal cancer is well established with tobacco. The present study is conducted in demographic belt in West India where tobacco consumption is higher than the national average, and hence, laryngeal cancer is an important ailment in the given demographics.[1],[2]
Laryngeal cancer is a potentially treatable disease, and it is one of the few malignancies where a surgical approach is not a primary treatment protocol and is reserved for the locally advanced disease. After the 1991 publication of the veterans administration (VA) laryngeal trial,[3] a paradigm shift came in the treatment protocol of laryngeal cancer. Where before that time, a total laryngectomy was the primary treatment for most patients with T3–T4 laryngeal cancer, after that trial organ preservation along with more conservative treatment such as concurrent chemoradiotherapy was started to be preferred as the first-line treatment.[4]
Thyroid cartilage invasion has been defined as one of the crucial criteria which determine the need for total laryngectomy in a case of laryngeal cancer. According to the current American Joint Committee on Cancer guidelines, where a minor cartilage involvement defines T3 disease which may be treated with an organ preservation approach, a major thyroid cartilage erosion or destruction defines T4 disease which warrants for a more radical surgical approach. Although a number of recent trials suggest possible roles of chemoradiotherapy even in advanced stages, it is yet to be accepted as a primary treatment protocol in most institutions including ours.[4],[5],[6]
In the present era, multidetector computed tomography (MDCT) forms the backbone of head and neck oncological imaging due to its superior accuracy in detection of various parameters such as soft-tissue lesions, underlying bony involvements, better depiction of nodal status, and comprehensive approach in detecting disease extension due to its multiplanar reconstructive capability. In addition, phonation and Valsalva maneuver imaging help detect the presence and extent of smaller glottic lesions.[7]
However, MDCT has long been accused of a less accurate analysis of the thyroid cartilage involvement in laryngeal cancer by often overestimating the cartilage involvement. The MDCT results may lead to a clinicoradiological dilemma which often results in the patient being over staged and hence subjected to surgery whereas a more accurate preoperative staging could have helped treat the patient with organ preservation techniques.[8]
The present study is conducted to address this constant dilemma and aims at analyzing the accuracy of MDCT in detecting thyroid cartilage invasion in laryngeal and hypopharyngeal cancer in a tertiary center. The MDCT results were compared with histopathological examination (HPE) results which were considered as gold standard.
Materials and Methods
The present study was conducted in a tertiary hospital in Western India which is located in a high tobacco consumption belt.
Study design
After due Institutional Ethical Committee approval, a retrospective analysis was done for patients presenting as T3 and T4 stage of laryngeal and hypopharyngeal cancers in the tertiary teaching institute from April 2016 to March 2017.
The study comprised of patients who were clinically and radiologically diagnosed as T3/T4 laryngeal or hypopharyngeal disease and underwent laryngectomy and HPE evaluation at our institute. The postoperative HPE results were reviewed for each patient and were taken as gold standard for evaluation of the accuracy of MDCT in detecting preoperative thyroid cartilage involvement.
We excluded the patients from our study who did not undergo laryngectomy at our institute. Furthermore, the patients who had taken chemotherapy or radiotherapy before the surgery were excluded from our study.
The MDCT results were retrospectively reviewed by a single radiologist (the author) who was blind to the pathological diagnosis. The histopathological results were obtained from the hospital's database and reviewed to be compared with MDCT results.
Multidetector computed tomography protocol and result analysis
Protocol
The study was performed with a 128 Slice Optima CT 660 (Wipro GE Healthcare Pvt. Ltd.) machine. The procedure was briefly explained to the patient, and detailed informed consent was obtained. An initial topogram of the neck was obtained, and further series were planned accordingly. With the patient in supine position, noncontrast 5 mm thick contiguous axial MDCT sections of the neck were performed from the skull base to aortic arch, subsequently followed by intravenous administration of 80 ml nonionic iodinated contrast medium (300 mg iodine/ml - iohexol) using an automated power injector. Phonation images were acquired subsequently. The axial images were reconstructed to procure sagittal and coronal reformations of high quality, with reconstructed sections as thin as 1.25 mm obtained through the region of interest.
Multidetector computed tomography analysis
The analysis aimed to establish the efficacy of MDCT comprehensively in detecting thyroid cartilage invasion in its various stages, thereby staging laryngeal cancer along with the individual accuracy of various appearances of the involved cartilage in demarcating the disease stage.
Cartilage involvement
The results of thyroid cartilage assessment were marked as no involvement, minor involvement, and major involvement.
Cortical irregularity and erosion of only inner cortex were considered minor involvement. Asymmetrical sclerosis, erosion through both inner and outer cortices, lysis, and presence of enhancing lesion on both sides of cartilage depicting extralaryngeal spread through the cartilage were considered the criteria for major cartilage erosion.[5]
Minor cartilage involvement was seen as a depicter of T3 disease while major cartilage erosion was considered as a marker of T4 disease.[2],[4] Criteria are schematically depicted in [Figure 1].
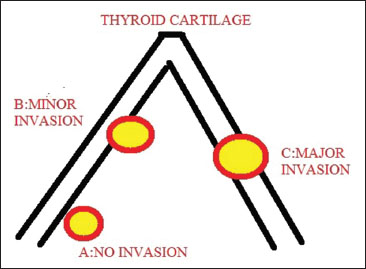
| Figure. 1Schematic diagram depicting types of thyroid cartilage involvement in laryngeal cancer
Histopathological evaluation
The histopathological results after total laryngectomy were reported as no involvement, superficial involvement, and cartilage involvement by the institute's Pathology Department.
Statistical analysis
Statistical analysis was made using Microsoft Excel and MedCalc Software. The results of MDCT in evaluating various types of cartilage involvement in comparison to the corresponding pathological diagnosis were calculated in terms of sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV).
It is prudent to understand that this study is aimed at addressing the clinicoradiological tussle over the overdiagnosis of cartilage invasion by MDCT in laryngeal cancer and not regarding the primary pick up ability of MDCT in this situation; therefore, while analyzing the statistical data, it is the PPV and NPV of MDCT that takes the front seat rather than sensitivity and specificity.[8]
Results
On retrospective analysis of data, we found that 61 cases of laryngeal or hypopharyngeal carcinoma had presented to our department for MDCT neck evaluation in the given time. Out of this 61, 22 cases fulfilled our inclusion criteria and were included in the study.
Demographics
The study group demographic profile is depicted in [Table 1] and [Table 2].
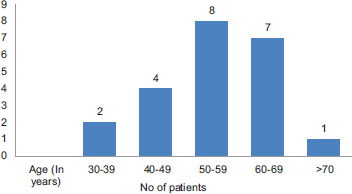
| Table. 1Age distribution
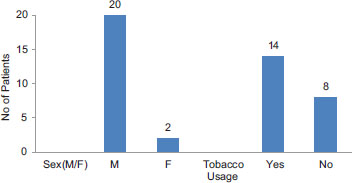
| Table. 2Sex distribution and association with tobacco usage
Supraglottic involvement was the most common presentation seen in 72.72% patients. Most cases presented with laryngeal component of disease, only two cases (9.0%) showed hypopharyngeal involvement only with no laryngeal component [Table 3].
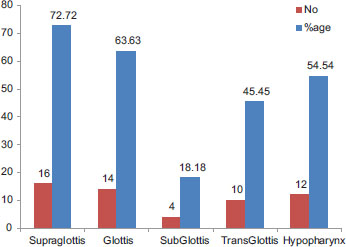
| Table. 3Primary site of involvement
Cartilage involvement
A total number of cartilages involved as seen by MDCT were 15 while only 10 were pathologically confirmed to be involved.
Computed tomography (CT) found minor cartilage erosion in only three cases out of which pathology confirmed superficial erosion in one case and no erosion in the remaining two cases. Major cartilage invasion as depicted by various findings as defined in the criteria above was found in 12 cases on MDCT. Out of these, eight cases were pathologically confirmed to have major thyroid cartilage invasion, and in four cases, the cartilage was found free from the lesion or to be having only superficial erosion. There was only one false-negative case in which cartilage invasion was confirmed on HPE but missed by MDCT.
The statistical results of MDCT in detecting minor and major cartilage involvement are depicted in [Table 4] and [Table 5].
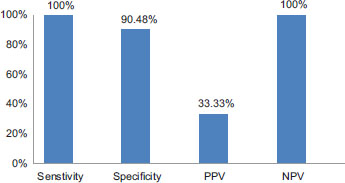
| Table. 4Statistical analysis of multidetector computed tomography results in detecting minor cartilage invasion
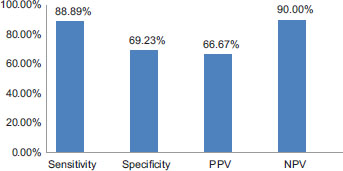
| Table. 5Statistical results of multidetector computed tomography in detecting major cartilage erosion
In analyzing accuracy of individual CT appearances of a major invasion as in erosion of both inner and outer cortices and lysis, we found that these features were shown in 11 cases on MDCT out of which 8 were pathologically confirmed to be T4A disease while the rest were downgraded to T3 disease by pathology. The presence of enhancing soft tissue on both sides of the thyroid cartilage and extralaryngeal spread was seen in seven cases on MDCT out of which five were pathologically proven to be T4A disease and two were downgraded to T3 disease. Statistical results of individual morphological findings in depicting T4A staging are tabulated in [Table 6]. The overall results of MDCT in detecting all types of cartilage invasion are shown in [Table 7].
|
Morphological character on MDCT depicting major cartilage involvement |
TP |
TN |
FP |
FN |
Sensitivity (%) |
Specificity (%) |
PPV (%) |
NPV (%) |
|---|---|---|---|---|---|---|---|---|
|
Depicted as number of cases. MDCT – Multidetector computed tomography; PPV – Positive predictive value; NPV – Negative predictive value; TP – True positive; TN – True negative; FP – False positive; FN – False negative |
||||||||
|
Sclerosis |
2 |
6 |
1 |
9 |
18.18 |
85.71 |
66.67 |
40 |
|
Through and through invasion |
8 |
10 |
3 |
1 |
88.89 |
76.92 |
72.73 |
90.91 |
|
Extralaryngeal spread |
5 |
14 |
2 |
1 |
83.33 |
87.50 |
71.43 |
93.33 |
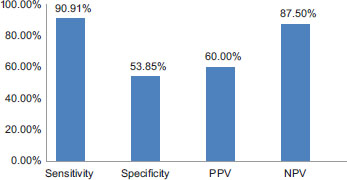
| Table. 7Final statistical results of multidetector computed tomography in detecting thyroid cartilage invasion (both minor and major)
Multidetector computed tomography in detecting stage of laryngeal cancer
It is important to remind that while thyroid cartilage invasion is a very important criteria for T-stage detection in laryngeal cancer, it is not the only criteria for demarking these two stages, and many other CT findings play a crucial role such as the involvement of preepiglottic and paraglottic areas in T3 disease and the invasion of strap muscles, the thyroid gland, and esophagus in T4A disease. Therefore, it is worthwhile to analyze the overall capacity of MDCT in detecting the disease stage which is ultimately the actual guide for therapeutic results.
It was observed that out of eight cases marked as T3 disease by MDCT, four were confirmed by pathology while the other four were downgraded to T2 disease by pathology. CT demarked 14 cases to be of T4A disease out of which 11 were confirmed by pathology and 3 were downgraded to T3 disease. A total of 7 out of 22 cases were downgraded in staging by pathology [Table 8].
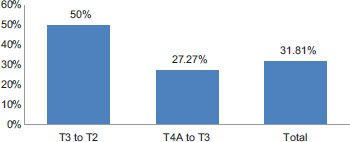
| Table. 8Accuracy of multidetector computed tomography in detecting T4A disease as compared to final histopathological results
Representative cases are depicted in [Figure 2] and [Figure 3].
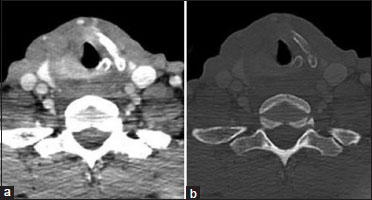
| Figure. 2(a) Axial contrast-enhanced computed tomography soft-tissue window images show enhancing lesion in the right glottis eroding through the right thyroid cartilage with extralaryngeal spread. (b) Bone window image shows complete lysis of the right lamina of thyroid cartilage. Major cartilage invasion was confirmed by histopathological examination in this case
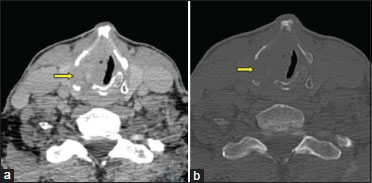
| Figure. 3(a) Axial contrast-enhanced computed tomography soft-tissue window shows enhancing mass lesion eroding through the right lamina of thyroid cartilage. (b) Bone window image shows a lytic defect in the right lamina of thyroid cartilage at this level. However, on histopathological examination, major cartilage invasion was not confirmed
Discussion
Laryngeal cancer forms about one-fourth of the diagnosed head and neck cancers in India. It has a strong male predominance as per the Indian Cancer Registries, being one of the top ten cancers to affect Indian men. In our study, we made a similar observation with 88% of the study group consisting of males. Similar observations were made by Sharif et al.[9] and by Bobdey et al.[1]
Laryngeal cancer is a disease of the elderly with most cases presenting between 50 and 70 years of age. The mean age in our study group was found to be 54.36 years. As depicted in literature, we also found a strong association with tobacco chewing in our study, in as many as 63.63% patients.[1],[2]
The current management protocol of advanced laryngeal cancer is guided by the American Joint Committee for Cancer which has made preoperative evaluation of laryngeal cancer, an essential requirement for the concerned oncologist, and a meticulous responsibility for the concerned radiologist. Major thyroid cartilage erosion defines T4 disease while Minor cartilage erosion defines T3 disease, both having different management protocols. It has been long established that a major thyroid cartilage erosion defines higher rate of recurrence and significantly reduces the chances of success of radiotherapy, thereby implying that only conservative measures will not suffice, and in this case, surgical treatment becomes a mandatory consideration subject to resectability.[2],[3],[4]
A vast window has been found in depicting the accuracy of CT in detecting thyroid cartilage involvement which ranges from 7% to 83% sensitivity and 40%–100% in the early studies conducted by Becker et al.[10] Over the years and even with the advent of various techniques, the variation still remains. In a recent study, Hartl et al.[11] found CT's sensitivity to be as low as 10.5% and PPV to be 13% in detecting thyroid cartilage involvement in mid to advanced laryngeal cancers.
In our study, we found that the PPV of CT was best in detecting major cartilage invasion, i.e., 66.67%, where a definite erosion of the outer cortex and extralaryngeal spread are helpful criteria for diagnosis. This was followed by the PPV for diagnosing all types of cartilage involvement, i.e., 60.00%. The major observation from this study was the poor results of CT in diagnosing minor cartilage erosion with a PPV of only 33.33%. The closest similarity with our study results was depicted by Li et al.[8] who also analyzed the involvement of cartilage on similar parameters of minor, major, and overall involvement [Table 9].
|
PPV in minor thyroid cartilage erosion |
PPV in major thyroid cartilage erosion |
PPV in overall thyroid cartilage erosion |
|
|---|---|---|---|
|
Present study (%) |
33.33 |
66.67 |
60.00 |
|
Study by Li et al. (%) |
30 |
78 |
63 |
| Figure. 1Schematic diagram depicting types of thyroid cartilage involvement in laryngeal cancer
| Table. 1Age distribution
| Table. 2Sex distribution and association with tobacco usage
| Table. 3Primary site of involvement
| Table. 4Statistical analysis of multidetector computed tomography results in detecting minor cartilage invasion
| Table. 5Statistical results of multidetector computed tomography in detecting major cartilage erosion
| Table. 7Final statistical results of multidetector computed tomography in detecting thyroid cartilage invasion (both minor and major)

| Table. 8Accuracy of multidetector computed tomography in detecting T4A disease as compared to final histopathological results

| Figure. 2(a) Axial contrast-enhanced computed tomography soft-tissue window images show enhancing lesion in the right glottis eroding through the right thyroid cartilage with extralaryngeal spread. (b) Bone window image shows complete lysis of the right lamina of thyroid cartilage. Major cartilage invasion was confirmed by histopathological examination in this case
| Figure. 3(a) Axial contrast-enhanced computed tomography soft-tissue window shows enhancing mass lesion eroding through the right lamina of thyroid cartilage. (b) Bone window image shows a lytic defect in the right lamina of thyroid cartilage at this level. However, on histopathological examination, major cartilage invasion was not confirmed
References
- obdey S, Jain A, Balasubramanium G. Epidemiological review of laryngeal cancer: An Indian perspective. Indian J Med Paediatr Oncol 2015; 36: 154-60
- oshi VM, Wadhwa V, Mukherji SK. Imaging in laryngeal cancers. Indian J Radiol Imaging 2012; 22: 209-26
- fister DG, Strong E, Harrison L, Haines IE, Pfister DA, Sessions R. et al. Larynx preservation with combined chemotherapy and radiation therapy in advanced but resectable head and neck cancer. J Clin Oncol 1991; 9: 850-9
- eitler JJ, Muller S, Grist WJ, Corey A, Klein AM, Johns MM. et al. Prognostic accuracy of computed tomography findings for patients with laryngeal cancer undergoing laryngectomy. J Clin Oncol 2010; 28: 2318-22
- heahan P. Management of advanced laryngeal cancer. Rambam Maimonides Med J 2014; 5: e0015
- d">6 Karatzanis AD, Psychogios G, Waldfahrer F, Kapsreiter M, Zenk J, Velegrakis GA. Management of locally advanced laryngeal cancer. J Otolaryngol Head Neck Surg 2014; 43: 4
- onnor S. Laryngeal cancer: How does the radiologist help?. Cancer Imaging 2007; 7: 93-103
- i B, Bobinski M, Gandour-Edwards R, Farwell DG, Chen AM. Overstaging of cartilage invasion by multidetector CT scan for laryngeal cancer and its potential effect on the use of organ preservation with chemoradiation. Br J Radiol 2011; 84: 64-9
- harif KS, Malek M, Mazaher H, Sharifi anH. The diagnostic accuracy of computed tomography in neoplastic invasion of the laryngeal cartilage. Iran J Radiol 2008; 5: 11-17
- Becker M, Zbären P, Delavelle J, Kurt AM, Egger C, Rüfenacht DA. et al. Neoplastic invasion of the laryngeal cartilage: Reassessment of criteria for diagnosis at CT. Radiology 1997; 203: 521-32
- Hartl DM, Landry G, Bidault F, Hans S, Julieron M, Mamelle G. et al. CT-scan prediction of thyroid cartilage invasion for early laryngeal squamous cell carcinoma. Eur Arch Otorhinolaryngol 2013; 270: 287-91
- d">12 Adolphs AP, Boersma NA, Diemel BD, Eding JE, Flokstra FE, Wegner I. et al. Asystematic review of computed tomography detection of cartilage invasion in laryngeal carcinoma. Laryngoscope 2015; 125: 1650-5
- d">13 Koopmann M, Weiss D, Steiger M, Elges S, Rudack C, Stenner M. Thyroid cartilage invasion in laryngeal and hypopharyngeal squamous cell carcinoma treated with total laryngectomy. Eur Arch Otorhinolaryngol 2016; 273: 3789-94
- d">14 Fernandes R, Gopalan P, Spyridakou C, Joseph G, Kumar M. Predictive indicators for thyroid cartilage involvement in carcinoma of the larynx seen on spiral computed tomography scans. J Laryngol Otol 2006; 120: 857-60
- Scarfe WC, Farman AG. Soft tissue calcifi cations in the neck: Maxillofacial CBCT presentation and signifi cance. Austr Dent Pract 2008; 19: 102-8
- Zbären P, Becker M, Läng H. Staging of laryngeal cancer: Endoscopy, computed tomography and magnetic resonance versus histopathology. Eur Arch Otorhinolaryngol 1997; 254 Suppl 1: S117-22
- Jain SN, Varma R. Imaging in laryngeal tumors. Otorhinolaryngol Clin Int J 2010; 2: 167-74
- Kuno H, Onaya H, Iwata R, Kobayashi T, Fujii S, Hayashi R. Evaluation of cartilage invasion by laryngeal and hypopharyngeal squamous cell carcinoma with dual-energy CT. Radiology 2012; 265: 488-96