 PDF
PDF  Views
Views  Share
Share


Posterior reversible encephalopathy syndrome in pediatric acute leukemia: Case series and literature review
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2014; 35(01): 79-82
DOI: DOI: 10.4103/0971-5851.133727
Abstract
Posterior reversible encephalopathy syndrome (PRES) is a neurotoxic state coupled with a unique radio imaging appearance. We describe this rare, mostly reversible condition in five cases undergoing similar treatment under preset protocol (MCP-841) for acute lymphoblastic leukemia (ALL) at our centre. Hypertension is a well-known adverse effect of high-dose corticosteroid therapy primarily mediated by its effects on the mineralocorticoid receptor especially in pediatric population and we hypothesize that this may be the etiology of PRES in two of these patients.
Publication History
Article published online:
19 July 2021
© 2014. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Posterior reversible encephalopathy syndrome (PRES) is a neurotoxic state coupled with a unique radio imaging appearance. We describe this rare, mostly reversible condition in five cases undergoing similar treatment under preset protocol (MCP-841) for acute lymphoblastic leukemia (ALL) at our centre. Hypertension is a well-known adverse effect of high-dose corticosteroid therapy primarily mediated by its effects on the mineralocorticoid receptor especially in pediatric population and we hypothesize that this may be the etiology of PRES in two of these patients.
INTRODUCTION
The use of corticosteroids with other cytotoxic drugs in clinical oncology is widespread and customary adverse effects of their use are well known. We describe here a presentation of posterior reversible encephalopathy syndrome (PRES) — a rare, mostly reversible complication of possible corticosteroid therapy in two cases and unknown mostly attributable to cytotoxics used in other three cases. The common presentations noted in these five patients were hypertension, visual disturbances, seizures, and altered sensorium while on induction phase (A) treatment of MCP-841 protocol with prednisolone (40 mg/m2), vincristine (1.4 mg/m2), doxorubicin (30 mg/m2), L asparginase (60 mg/m2) and intrathecal methotrexate for acute lymphoblastic leukemia and lymphoma. With conservative management, four patients had complete recovery of their neurological symptoms within a few days, while one patient succumbed to death due to coexisting comorbidities.
PRES is a rare condition with only a few cases described in western and Indian literature, the incidence is even lesser in patients receiving chemotherapy.
CASE REPORT
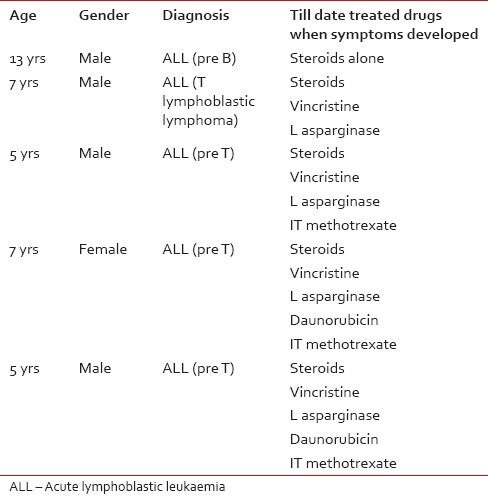
We report five cases that occurred between 2009 and 2012 at department of pediatric oncology, Kidwai Memorial Institute of Oncology, wherein four were males and one was a female. Among them, four patients were diagnosed as acute lymphoblastic leukemia while one was a case of acute lymphoblastic lymphoma. However, all received MCP-841 protocol and were in varying periods of induction with mentioned cytotoxics when complication was noted [Table 1].
Table 1
Induction drug schedule of patients
|
Case 1
A 13 year male diagnosed as ALL L1/L2 (immunophenotyping not introduced at that time) in May 2009. He was planned on MCP-841 protocol and started on steroids. He was continued on steroids alone as his performance status was poor to initiate other cytotoxics of regime. Day 20 of steroids he developed seizures (GTCS). He was normotensive on examination with altered sensorium. Labs — hemogram showed platelet count of 20000 cells/mm3, rest of hemogram parameters, biochemical and metabolic workup were normal. MRI brain showed B/L occipital lobe hypo density suggestive of PRES. He was started on antiepileptics, no further seizures were reported. ALL protocol was restarted after 10 days.
Case 2
A 7 year male was diagnosed as T acute lymphoblastic lymphoma in July 2010 and was initiated on MCP-841 protocol. He developed hypersensitivity reaction to first dose of L asparginase and hence further doses were stopped. D 6 of induction on steroids, post one dose VCR and one IT MTX, he developed seizures associated with blurring of vision and altered sensorium. On examination, he was hypertensive (BP 130/100 mm Hg), fundus revealed grade II hypertensive retinopathy. Labs showed normal hemogram, biochemistry, and electrolytes. Workup for other causes of HTN- cardiac ECHO, USG abdomen, renal Doppler, urine routine were all normal. MRI brain showed B/L frontal and parietal hypo densities S/O PRES. He was started on antihypertensives and antiepileptics with regular monitoring of blood pressure and titration of antihypertensives (amlodipine, atenolol, and prazosin) accordingly. He became asymptomatic in 10 days with normalization of blood pressure and protocol was resumed.
Case 3
A 5 year male patient was diagnosed as T ALL in April 2010 and initiated on MCP-841 protocol. Day 7 post induction when he had received 3 doses of L asparginase, one VCR, one IT MTX and on continued steroids, he developed seizures. He was normotensive. Labs — hemogram normal except platelet count of 75000 cells/mm3, biochem and electrolytes were normal. MRI brain showed B/L parieto-occipital and fronto-parietal cortical/subcortical T2 hyperintensities with no evidence of diffusion restriction S/O PRES (as depicted in Figures Figures11 and and22 of image section). He was started on antiepileptics, resumed ALL treatment after 1 week and completed uneventfully.
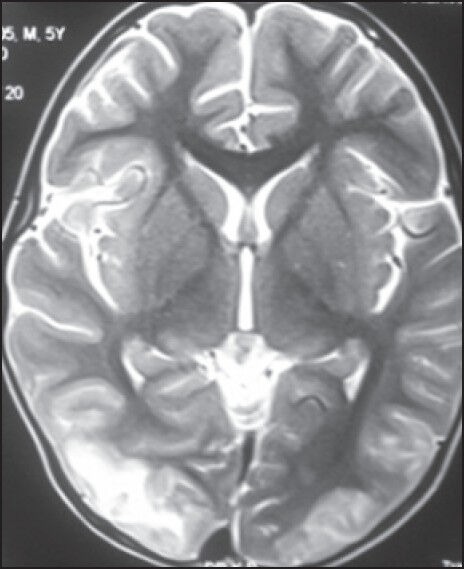
| Figure 1:This depicts a 5yr old patients T2w axial section at the level of basal ganglia showing illdefined hyperintensities in right parietooccipital, cortical and subcortical white matter
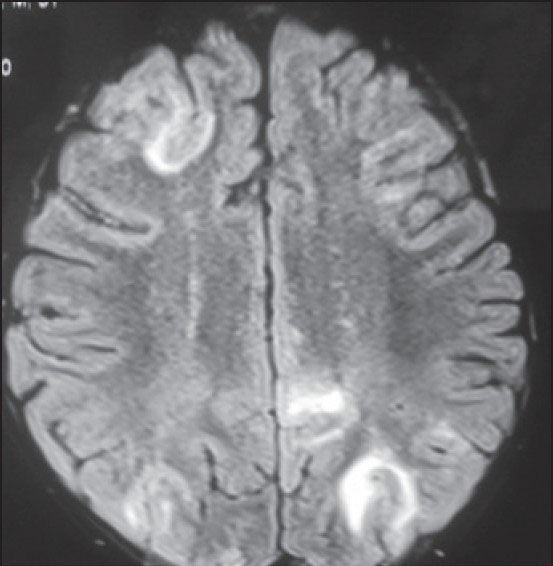
| Figure 2:The same patients FLAIR sequence at the level of centrum semiovale shows subcortical hyperintensities in right frontal and bilateral parietooccipital regions with no evidence of diffusion restriction. The typical appearance and distribution of lesions suggests a possibility of PRESS
Case 4
A 5 year male, diagnosed as T ALL in march 2012 and started on MCP-841 protocol, completed induction 1 and was on tapering steroid dose when he developed seizures with altered sensorium. On examination, he was normotensive with labs showing Hb 7 gm/dl, TC 2000 cells/mm3, platelet count 45000 cells/mm3, rest biochem and electrolytes were normal. MRI brain — hyper intense in FLAIR sequence along periventricular, RT frontal, B/L parieto-occipital region S/O PRES. He was started on antiepileptics and other supportive measures. Day 19 he died of a massive GIT bleeding.
Case 5
A 7 year female, diagnosed as T All in July 2012 was started on MCP 841 protocol. Day 10 — post four L asparginase, two VCR, one duanomycin, two IT MTX, and continued steroids. She developed seizures with altered sensorium. On examination she was hypertensive (BP 150/90 mm Hg), fundoscopy normal. Labs — hemogram, biochem, electrolytes within normal limits. MRI brain — T1 hyper/T2 flair hyper intensity in left parieto occipital region with diffusion restriction S/O PRES.
She was started on antiepileptics and antihypertensives (amlodipine). She recovered in 12 days and protocol resumed.
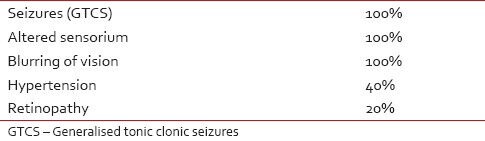
The most common presentation [Table 2] in all patients was with generalized clonic tonic seizure (100%) which was managed with parenteral phenytoin loading of 15 mg/kg followed by maintenance with oral phenytoin at 4-5 mg/kg. Clinical examination in all revealed no neurological deficits. Seizures were associated with altered sensorium which persisted from a minimum of 1 day to a maximum of 10 days for which antiedema measures were started.
Table 2
Clinical features
|
The next common manifestation was hypertension seen in two (40%) patients, which was attributed to steroids. They were initiated on antihypertensives as mentioned in individual case reports along with fluid and salt restriction. Blood pressure was carefully monitored and antihypertensive dose titrated. Blood pressure normalized within a few days, ranging from 10 days to 2 weeks. Among the two, one developed GRADE II HYPERTENSIVE RETINOPATHY, which stabilized following normalization of blood pressure.
MRI brain [Table 3, Figures Figures11 and and2]2] with contrast was done in all five patients which showed T2 FLAIR hyperintensities with no evidence of diffusion restriction in parieto-occipital area (80%), occipital only (20%), frontal and parieto occipital lesions (40%).
Table 3
MRI brain imaging findings

|
Among them, four patients had uneventful recovery with three patients having completed scheduled treatment. One patient died, which followed massive gastrointestinal bleeding. A repeat MRI at the end of induction (day 30) was normal in all four patients. Based on clinical presentation, imaging appearance, and complete restoration of symptoms, a diagnosis of PRES was made.
Etiopathogenesis
The exact mechanism of PRES is unclear and seems to be multifactorial. Hypertension is likely to play a major role and its treatment is likely to have a favorable outcome.[1] Hinchey et al. described this condition and suggested that PRES represented a localized manifestation of hypertensive encephalopathy occurring secondary to hypertensive crisis.[2] PRES has been described in several conditions including eclampsia,[3] infections,[4] dyselectrolemia i.e. hypercalcemia,[5] and drugs like immunosuppressive therapy, erythropoietin, interferon alfa, cytotoxic chemotherapy (cyclophosphamide), molecular-targeted agents such as sorafenib and bevacizumab used in hemato-oncology.
Three theories have been postulated for development of PRES. The earliest theory suggested that overreaction of brain auto regulation results in reversible vasospasm, which in turn results in potentially reversible ischemia to the brain, especially in vascular border zone territories. A newer theory suggests that auto regulation maintains a constant blood flow to the brain despite systemic blood pressure alterations by means of arteriolar constriction and dilatation. The constricted arterioles are forced to dilate because of the increased systemic blood pressure, resulting in brain hyper fusion. This increased perfusion pressure is sufficient to overcome the blood-brain barrier, allowing extravasion of fluid, macromolecules into the brain parenchyma. So, PRES represents vasogenic rather than cytotoxic edema in the majority of cases.[6] The last theory suggests that at intravascular pressures just below those that could rupture the capillary wall, permeability through the endothelium increases markedly, due to increased pinocytotic activity. The active passage of fluid through the capillary wall may act to relieve intravascular pressure, forestalling the development of large hemorrhages. This is more commonly seen in posterior brain regions due to a sparse sympathetic innervation of the vertebrobasilar vascular system i.e. Watershed area.[7]
Clinical features
The clinical presentation includes headache, seizures, visual disturbances (including cortical blindness and visual hallucinations), and alterations in mental status.[8] Lethargy and somnolence are often the first signs noted. Visual abnormalities appear later. Hypertension is typically present, though some patients with PRES can be normotensive also. Clinical examination findings are relatively unimpressive, with the exception of brisk deep tendon reflexes (particularly of the lower extremities) and extensor plantar responses. PRES is also well recognized in the settings of stem cell transplantation.[9] The incidence of PRES after allo-BMT using myeloablative marrow preconditioning and cyclosporine immune suppression is approximately 7-9%, seen commonly in the first month. It is usually reversible in majority of cases; however, case reports of atypical presentations with irreversible neurodeficits and encephalomalacia have been reported.[10]
Diagnosis and management
MRI remains the diagnostic modality of choice. MRI of the brain demonstrates hyper intense lesions of the white matter and adjacent gray matter of fluid attenuation inversion recovery and T2-weighted images located in the occipital and posterior parietal lobes. Involvement of other areas of the brain is less frequently reported.[11] At imaging, vasogenic edema is greater in normotensive patients than in severely hypertensive patients. On MR angiography (MRA), a reversible “vasculopathy” (diffuse/focal vasoconstriction) or vessel pruning is noted. Diffusion weighted imaging can differentiate this condition from ischemic/cytotoxic edema. Differential diagnosis includes PCA territory infarcts, venous thrombosis, demyelinating disorders, and encephalitis.
DISCUSSION
PRES is a neurotoxic state coupled with a unique MR imaging appearance. Hypertension is believed to be the unifying precipitant in many cases, but it does occur in normotensives also. Various theories have been proposed but exact mechanism remains to be elucidated. Hypertension is a well-known adverse effect of corticosteroid therapy primarily mediated by its effects on the mineralocorticoid receptor, and we hypothesize that this may be the etiology of PRES in these patients but implication of the other cytotoxic drugs cannot be excluded. It should be emphasized that blood pressure should be routinely monitored when on steroids. Given the widespread use of steroids in the field of oncology, it is important to recognize PRES as a rare but usually reversible complication, especially in pediatric patients receiving treatment for acute lymphoblastic leukemia and appropriate treatment should be initiated accordingly after ruling out other causes which could result in a similar clinical presentation like cortical venous thrombosis, CNS hemorrhage, CNS leukemic infiltration, and encephalitis.
Footnotes
Source of Support: Sincere thanks to Dr. Kavitha Srivastha and Dr. Avinash T, faculty Dept. of Pediatric oncology for their support.
Conflict of Interest: None declared.
References
- Ozcakar ZB, Ekim M, Fitoz S, Teber S, Hizel S, Acar B, et al. Hypertension induced reversible posterior leukoencephalopathy syndrome: A report of two cases. Eur J Pediatr 2004;163:728-30.
- Hinchey J, Chaves C, Appignani B, Breen J, Pao L, Wang A, et al. A Reversible posterior leucoencephalopathy Syndrome. N Engl J Med 1996;334:494-500.
- Naheedy MH, Biller J, Schiffer M, Azar-Kia B, Gianopoulous J, Zarandy S. Toxemia of pregnancy: Cerebral CT findings. J Comput Assist Tomogr 1985;9:497-501.
- Bartynski WS, Boardman JF, Zeigler ZR, Shadduck RK, Lister J. Posterior reversible encephalopathy syndrome in infection, sepsis and shock. AJNR Am J Neuroradiol 2006;27:2179-90.
- Kastrup O, Maschke M, Wanke I, Diener HC. Posterior Reversible Encephalopathy Syndrome due to Hypercalcemia. J Neurol 2002;249:1563-6.
- Schaefer PW, Buonanno FS, Gonzalez RG. Diffusion-weighted imaging discriminates between cytotoxic and vasogenic edema in a patient with eclampsia. Stroke 1997;28:1082-5.
- Bartynski WS, Grabb BC, Zeigler Z. Watershed imaging features clinical vascular injury in cyclosporin a neurotoxicity. J Comput Assist Tomogr 1997;21:872-80.
- Kwon S, Koo J, Lee S. Clinical spectrum of reversible posterior leukoencephalopathy syndrome. Pediatr Neurol 2001;24:361-4.
- Moskowitz A, Nolan C, Lis E, Castro-Malaspina H, Perales MA. Posterior reversible encephalopathy syndrome due to sirolimus. Bone Marrow Transplant 2007;39:653-4.
- Komur M, Delibas A, Arslankoylu AE, Okuyaz C, Kara E. Recurrent and atypical posterior reversible encephalopathy syndrome in a child with hypertension. Ann Indian Acad Neurol 2012;15:208-10.
- McKinney AM, Short J, Truwit CL, McKinney ZJ, Kozak OS, SantaCruz KS, et al. Posterior reversible encephalopathy syndrome: Incidence of atypical regions of involvement and imaging findings. AJR Am J Roentgenol 2007;189:904-12.
| Figure 1:This depicts a 5yr old patients T2w axial section at the level of basal ganglia showing illdefined hyperintensities in right parietooccipital, cortical and subcortical white matter
| Figure 2:The same patients FLAIR sequence at the level of centrum semiovale shows subcortical hyperintensities in right frontal and bilateral parietooccipital regions with no evidence of diffusion restriction. The typical appearance and distribution of lesions suggests a possibility of PRESS
References
- Ozcakar ZB, Ekim M, Fitoz S, Teber S, Hizel S, Acar B, et al. Hypertension induced reversible posterior leukoencephalopathy syndrome: A report of two cases. Eur J Pediatr 2004;163:728-30.
- Hinchey J, Chaves C, Appignani B, Breen J, Pao L, Wang A, et al. A Reversible posterior leucoencephalopathy Syndrome. N Engl J Med 1996;334:494-500.
- Naheedy MH, Biller J, Schiffer M, Azar-Kia B, Gianopoulous J, Zarandy S. Toxemia of pregnancy: Cerebral CT findings. J Comput Assist Tomogr 1985;9:497-501.
- Bartynski WS, Boardman JF, Zeigler ZR, Shadduck RK, Lister J. Posterior reversible encephalopathy syndrome in infection, sepsis and shock. AJNR Am J Neuroradiol 2006;27:2179-90.
- Kastrup O, Maschke M, Wanke I, Diener HC. Posterior Reversible Encephalopathy Syndrome due to Hypercalcemia. J Neurol 2002;249:1563-6.
- Schaefer PW, Buonanno FS, Gonzalez RG. Diffusion-weighted imaging discriminates between cytotoxic and vasogenic edema in a patient with eclampsia. Stroke 1997;28:1082-5.
- Bartynski WS, Grabb BC, Zeigler Z. Watershed imaging features clinical vascular injury in cyclosporin a neurotoxicity. J Comput Assist Tomogr 1997;21:872-80.
- Kwon S, Koo J, Lee S. Clinical spectrum of reversible posterior leukoencephalopathy syndrome. Pediatr Neurol 2001;24:361-4.
- Moskowitz A, Nolan C, Lis E, Castro-Malaspina H, Perales MA. Posterior reversible encephalopathy syndrome due to sirolimus. Bone Marrow Transplant 2007;39:653-4.
- Komur M, Delibas A, Arslankoylu AE, Okuyaz C, Kara E. Recurrent and atypical posterior reversible encephalopathy syndrome in a child with hypertension. Ann Indian Acad Neurol 2012;15:208-10.
- McKinney AM, Short J, Truwit CL, McKinney ZJ, Kozak OS, SantaCruz KS, et al. Posterior reversible encephalopathy syndrome: Incidence of atypical regions of involvement and imaging findings. AJR Am J Roentgenol 2007;189:904-12.