 PDF
PDF  Views
Views  Share
Share


Pneumomediastinum and Subcutaneous Emphysema in the Neck, Axilla, and Chest Regions in a Patient with Olfactory Neuroblastoma Treated with Chemoradiotherapy
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2018; 39(04): 524-526
DOI: DOI: 10.4103/ijmpo.ijmpo_85_17
Abstract
Spontaneous pneumomediastinum and subcutaneous emphysema in the neck, axilla, and chest do not commonly occur after neoadjuvant cisplatin/etoposide chemotherapy, followed by radiotherapy, and adjuvant cisplatin/etoposide chemotherapy in patients with olfactory neuroblastoma. There are few case reports of pneumomediastinum induced by and occurring during bleomycin/etoposide/cisplatin chemotherapy in testicular cancer. The present case differs from the previous cases in that our patient developed spontaneous pneumomediastinum and subcutaneous emphysema in the neck, axilla, and chest approximately 2 months after completion of chemoradiotherapy for olfactory neuroblastoma. These conditions may have been treatment induced or caused by breath-holding after forceful inspiration. The latter would have created a massive pressure gradient between the alveoli and surrounding structures, causing alveolar rupture, and subsequent passage of air into the mediastinum and subcutaneous tissue of the neck, axilla, and chest.
Publication History
Article published online:
17 June 2021
© 2018. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Spontaneous pneumomediastinum and subcutaneous emphysema in the neck, axilla, and chest do not commonly occur after neoadjuvant cisplatin/etoposide chemotherapy, followed by radiotherapy, and adjuvant cisplatin/etoposide chemotherapy in patients with olfactory neuroblastoma. There are few case reports of pneumomediastinum induced by and occurring during bleomycin/etoposide/cisplatin chemotherapy in testicular cancer. The present case differs from the previous cases in that our patient developed spontaneous pneumomediastinum and subcutaneous emphysema in the neck, axilla, and chest approximately 2 months after completion of chemoradiotherapy for olfactory neuroblastoma. These conditions may have been treatment induced or caused by breath-holding after forceful inspiration. The latter would have created a massive pressure gradient between the alveoli and surrounding structures, causing alveolar rupture, and subsequent passage of air into the mediastinum and subcutaneous tissue of the neck, axilla, and chest.
Introduction
Bleomycin-induced pneumomediastinum in testicular cancer has been reported,[1] as has pneumomediastinum, subcutaneous emphysema, and pneumothorax after pulmonary function testing (the Valsalva maneuver) in a patient with bleomycin-induced interstitial pneumonitis.[2] Herein, we describe and radiologically document pneumomediastinum and subcutaneous emphysema in the neck, axilla, and chest 2 months after cisplatin/etoposide chemotherapy and radiotherapy in a patient with olfactory neuroblastoma.
Case Report
A 45-year-old man presented with nasal bleeding for 2 months. Local examination and computed tomography (CT) scan revealed a mass in the right side of the nasopharynx extending to the posterior nasal cavity. The mass was diagnosed as an olfactory neuroblastoma through immunohistochemistry of a biopsy specimen of the primary mass. Complete blood counts, random blood sugar levels, and liver and renal function tests were within normal limits. A chest X-ray (posteroanterior view), abdomen/pelvis ultrasound, and 12-lead electrocardiography showed no other abnormalities.
The patient received neoadjuvant chemotherapy with etoposide (100 mg, days 1–3) and cisplatin (40 mg, days 1–3) every 21 days for 2 cycles followed by external beam radiotherapy (70 Gy in 35 fractions for 7 weeks). Twenty-eight days after completion of radiotherapy, the chemotherapy was repeated (every 21 days for 4 cycles). The patient visited the radiotherapy department 13 days after treatment completion ( first follow-up). He was asymptomatic, with no evidence of residual local disease.
Two months after treatment completion (second follow-up), the patient presented with breathlessness. Chest X-ray (posteroanterior view) [Figure 1] and CT of the neck and chest showed extensive subcutaneous emphysema in the neck and axilla extending to the mediastinum [Figure 2]. He was referred to the chest unit where an intercostal drain (ICD) was inserted. The ICD relieved the pneumomediastinum and subcutaneous emphysema, and the patient was symptomatically better. After withdrawing the ICD, he was discharged from hospital. One week later, he died suddenly at home after an attack of coughing.

| Figure 1:A chest X-ray (posteroanterior view) showing subcutaneous emphysema in the neck
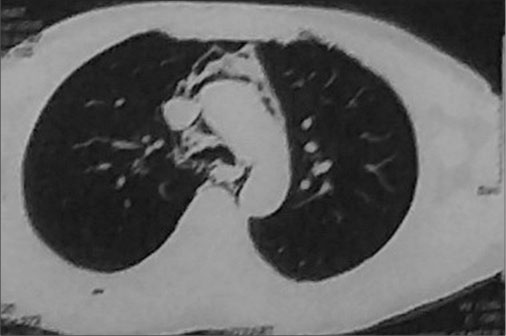
| Figure.2:Computed tomography of the neck and chest showed extensive subcutaneous emphysema in the neck and axilla extending to the mediastinum
Discussion
The visceral space, which is continuous from the neck and mediastinum to the retroperitoneum originates during embryological development.[3] The visceral pleura overlies both lungs in addition to the organs in the mediastinum and encloses a space known as the visceral cavity. The fascial planes connect cervical soft tissue to the mediastinum and retroperitoneum, and the spaces between the fasciae permit aberrant air arising in any of these areas to spread. In patients with pneumomediastinum, air can flow from the peribronchial space to the neck, chest wall, pleural cavity, mediastinum, retroperitoneum, pericardial cavity, pericardial space, and diaphragm.[3] Although the body cavity is further divided into thoracic, abdominal, and pericardial cavities by the pleuroperitoneal and pleuropericardial membranes, the cavities remain continuous throughout the visceral space.[4]
A chest X-ray usually detects pneumomediastinum and subcutaneous emphysema although better visualization is obtained through CT scan. In our case, CT scan showed extensive pneumomediastinum and subcutaneous emphysema. The patient underwent respiratory failure, which resulted in his death 2 months after the completion of treatment. The respiratory failure may have been chemotherapy drug induced or caused by forced expiration (e.g., the Valsalva maneuver with breath holding for a prolonged period).[2]
Spontaneous pneumomediastinum is an uncommon event characterized by retrosternal chest pain, subcutaneous emphysema, dyspnea, and dysphonia. Classic signs of pneumomediastinum include Hamman’s Crunch, a crepitant sound that varies with the heartbeat on auscultation of the precordium.[5] [6] Known triggers, which can be identified in some cases, include acute asthma exacerbation and the Valsalva maneuver; such complications are induced by structural changes associated with interstitial and other lung diseases. Other known triggers include those related to the Valsalva maneuver, sternuous exercise, weightlifting, inhalation of illicit drugs, coughing, forced evacuation, and labor as well as vomiting, respiratory infections, foreign body aspiration, and barotrauma. Pneumomediastinum usually follows a benign, self-limiting course.[5] [6]
Treatment of pneumomediastinum includes mediastinotomy and supportive care consisting of analgesic use, rest, and the avoidance of maneuvers that increase transpulmonary pressure (e.g., the Valsalva maneuver and spirometry). Radiotherapy is a treatment option for patients with prolonged air leaks who are not candidates for surgery.[7]
Our patient developed subcutaneous emphysema in the neck, axillary, and chest regions as well as pneumomediastinum and pneumothorax. He did not experience these complications during chemotherapy/radiotherapy and had no preexisting lung disease. An earlier study found that most air leak syndromes resulted from alveolar rupture rather than rupture of subpleural bullae.[8]
Intense respiratory efforts, adjacent atelectasis, and low intravascular pressure may contribute to the development of air leaks.[8] When a person inhales, the diameter of the pulmonary vein increases owing to a decrease in intrathoracic pressure and an increase in alveolar air volume and the venous return. Because all compartments increase in length and width in tandem, there is no pressure gradient in the interstitial space. However, when a person “holds his breath,” venous stasis occurs, which hinders pulmonary venous filling, reduces vessel lumen size, and consequently creates the pressure gradient necessary for alveolar rupture. The Valsalva maneuver is classically related to air leak syndromes because it increases intrapulmonary pressure.[8] Therefore, labor and forced evacuation are associated with pneumomediastinum.[8] Unreleased air pressure in the mediastinum can compress the heart and vessels and prevent lung inflation and deflation, resulting in death.
Conflict of Interest
There are no conflicts of interest.
References
- Noguchi G, Ota J, Ishigaki H, Onuki T, Kato Y, Moriyama M. A case of pneumomediastinum during BEP (bleomycin, etoposide, cisplatin) chemotherapy for testicular cancer. Hinyokika Kiyo 2013; 59: 545-9
- Araujo MS, Fernandes FL, Kay FU, Carvalho CR. Pneumomediastinum, subcutaneous emphysema, and pneumothorax after a pulmonary function testing in a patient with bleomycin-induced interstitial pneumonitis. J Bras Pneumol 2013; 39: 613-9
- Lee SY, Chen CH, Sheu CY, Tai JH, Yang SH, Chen CH. The radiological manifestations of the aberrant air surrounding the pleura: In the embryological view. Pulm Med 2012; 2012: 290802
- Sadler TW. Langman’s Medical Embryology. Baltimore, MD, USA: Williams & Wilkins; 1990
- Abolnik I, Lossos IS, Breuer R. Spontaneous pneumomediastinum. A report of 25 cases. Chest 1991; 100: 93-5
- Iyer VN, Joshi AY, Ryu JH. Spontaneous pneumomediastinum: Analysis of 62 consecutive adult patients. Mayo Clin Proc 2009; 84: 417-21
- Cetinkaya E, Ozgül MA, Gül S, Cam E, Büyükpolat Y. Treatment of a prolonged air leak with radiotherapy: A case report. Case Rep Pulmonol 2012; 2012: 158371
- Macklin MT, Macklin CC. Malignant interstitial emphysema of lungs and mediastinum as important occult complications in many respiratory diseases and other conditions: Interpretation of clinical literature in the light of laboratory experiment. Medicine 1944; 23: 281-358
Address for correspondence
Publication History
Article published online:
17 June 2021
© 2018. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2,
Noida-201301 UP, India
| Figure 1:A chest X-ray (posteroanterior view) showing subcutaneous emphysema in the neck
| Figure.2:Computed tomography of the neck and chest showed extensive subcutaneous emphysema in the neck and axilla extending to the mediastinum
References
- Noguchi G, Ota J, Ishigaki H, Onuki T, Kato Y, Moriyama M. A case of pneumomediastinum during BEP (bleomycin, etoposide, cisplatin) chemotherapy for testicular cancer. Hinyokika Kiyo 2013; 59: 545-9
- Araujo MS, Fernandes FL, Kay FU, Carvalho CR. Pneumomediastinum, subcutaneous emphysema, and pneumothorax after a pulmonary function testing in a patient with bleomycin-induced interstitial pneumonitis. J Bras Pneumol 2013; 39: 613-9
- Lee SY, Chen CH, Sheu CY, Tai JH, Yang SH, Chen CH. The radiological manifestations of the aberrant air surrounding the pleura: In the embryological view. Pulm Med 2012; 2012: 290802
- Sadler TW. Langman’s Medical Embryology. Baltimore, MD, USA: Williams & Wilkins; 1990
- Abolnik I, Lossos IS, Breuer R. Spontaneous pneumomediastinum. A report of 25 cases. Chest 1991; 100: 93-5
- Iyer VN, Joshi AY, Ryu JH. Spontaneous pneumomediastinum: Analysis of 62 consecutive adult patients. Mayo Clin Proc 2009; 84: 417-21
- Cetinkaya E, Ozgül MA, Gül S, Cam E, Büyükpolat Y. Treatment of a prolonged air leak with radiotherapy: A case report. Case Rep Pulmonol 2012; 2012: 158371
- Macklin MT, Macklin CC. Malignant interstitial emphysema of lungs and mediastinum as important occult complications in many respiratory diseases and other conditions: Interpretation of clinical literature in the light of laboratory experiment. Medicine 1944; 23: 281-358