 PDF
PDF  Views
Views  Share
Share


Patellar Metastasis in Renal Cell Carcinoma: A Rare Presentation
CC BY-NC-ND 4.0 ? Indian J Med Paediatr Oncol 2021; 42(06): 577-578
DOI: DOI: 10.1055/s-0041-1740139
A 61-year-old male underwent right-sided nephrectomy for renal cell carcinoma in June 2009. Histopathology showed conventional renal cell carcinoma, clear cell type, right kidney Fuhrman's nuclear grade II. He was staged to have pT3c N0 M0. In August 2018, he developed pulmonary metastasis (an irregular soft tissue lesion in the perihilar region of the right middle lobe) and nodal metastasis (multiple subcarinal and right hilar nodes). His IMDC (International Metastatic RCC Database Consortium) Risk Score was 0. He was started on Pazopanib (due to cost considerations) and was on regular follow-up. After 13 months of treatment with pazopanib (October 2019), he presented with pain in the right knee. X-ray of the right knee showed a lytic lesion in the patella ([Fig. 1]). MRI scan of the knee joint showed a well-defined, lobulated, altered marrow signal intensity lesion within the patella located superomedially. This lesion was appearing hypointense on T1 and intensely bright on T2 images. Restaging was not done as he did not have any other symptoms. Routine blood parameters were normal.
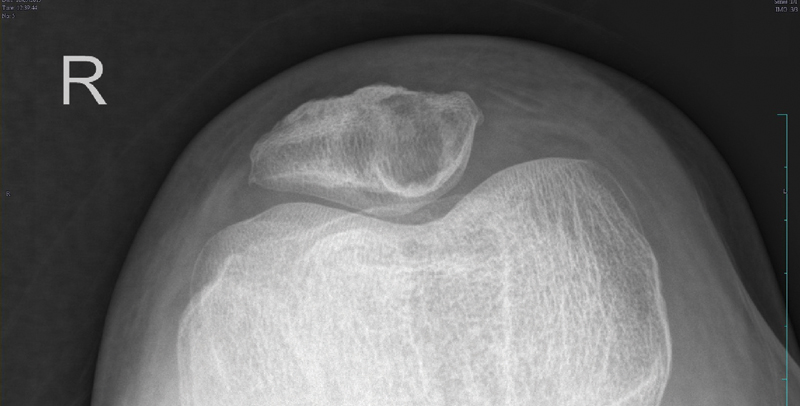
|?Fig. 1X-ray skyline view showing a lytic lesion in the patella.
He underwent curettage and bone cement application ([Fig. 2]). Histopathology from the right patellar lesion showed fibrocollagenous tissue with the presence of inflammatory cells and a neoplasm. The neoplasm was composed of clear cells arranged in nests. These clear cells were observed to be polygonal in shape and having a pale eosinophilic to clear cytoplasm and round to spindle-shaped hyperchromatic nuclei. Fibrovascular septae separated these nests. These findings were suggestive of metastatic clear cell carcinoma. He was given local radiation to the site with 20 Gy in five fractions, and pazopanib was continued. In January 2020, he became symptomatic with cerebral metastasis and was given whole-brain radiation for the same. He succumbed to his illness in November 2020.

|?Fig. 2X-ray lateral view showing lesion filled with bone cement.
Primary patellar tumors account for less than 1% of all bone tumors. Reports of metastatic lesions to the patella are even rarer. The rarity of patellar metastases is thought to be due to the patella's distal location and the relatively poor blood supply to the sesamoid bones. The most common primary tumor that usually metastasizes to the patella is lung carcinoma. Other metastasizing cancers are carcinomas of the breast, kidneys, esophagus, uterine cervix, cutaneous malignant melanoma, and head and neck.[1]
Fourteen percent of all patellar metastases were reported to arise from the kidneys in a case series.[2] Knee pain is a common clinical manifestation and can be associated with trauma or pathological fracture. Surgery can be offered if no other evidence of metastasis is seen elsewhere. However, bony metastasis from renal cell carcinoma appears to behave similarly to primary bone disease. Some experts believe there is no survival advantage by performing a wide resection in place of intralesional curettage and local stabilization.[2] The use of radiotherapy and bisphosphonates has also been advocated.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published, and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Publication History
10 December 2021 (online)
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
A 61-year-old male underwent right-sided nephrectomy for renal cell carcinoma in June 2009. Histopathology showed conventional renal cell carcinoma, clear cell type, right kidney Fuhrman's nuclear grade II. He was staged to have pT3c N0 M0. In August 2018, he developed pulmonary metastasis (an irregular soft tissue lesion in the perihilar region of the right middle lobe) and nodal metastasis (multiple subcarinal and right hilar nodes). His IMDC (International Metastatic RCC Database Consortium) Risk Score was 0. He was started on Pazopanib (due to cost considerations) and was on regular follow-up. After 13 months of treatment with pazopanib (October 2019), he presented with pain in the right knee. X-ray of the right knee showed a lytic lesion in the patella ([Fig. 1]). MRI scan of the knee joint showed a well-defined, lobulated, altered marrow signal intensity lesion within the patella located superomedially. This lesion was appearing hypointense on T1 and intensely bright on T2 images. Restaging was not done as he did not have any other symptoms. Routine blood parameters were normal.
|?Fig. 1X-ray skyline view showing a lytic lesion in the patella.
He underwent curettage and bone cement application ([Fig. 2]). Histopathology from the right patellar lesion showed fibrocollagenous tissue with the presence of inflammatory cells and a neoplasm. The neoplasm was composed of clear cells arranged in nests. These clear cells were observed to be polygonal in shape and having a pale eosinophilic to clear cytoplasm and round to spindle-shaped hyperchromatic nuclei. Fibrovascular septae separated these nests. These findings were suggestive of metastatic clear cell carcinoma. He was given local radiation to the site with 20 Gy in five fractions, and pazopanib was continued. In January 2020, he became symptomatic with cerebral metastasis and was given whole-brain radiation for the same. He succumbed to his illness in November 2020.
|?Fig. 2X-ray lateral view showing lesion filled with bone cement.
Primary patellar tumors account for less than 1% of all bone tumors. Reports of metastatic lesions to the patella are even rarer. The rarity of patellar metastases is thought to be due to the patella's distal location and the relatively poor blood supply to the sesamoid bones. The most common primary tumor that usually metastasizes to the patella is lung carcinoma. Other metastasizing cancers are carcinomas of the breast, kidneys, esophagus, uterine cervix, cutaneous malignant melanoma, and head and neck.[1]
Fourteen percent of all patellar metastases were reported to arise from the kidneys in a case series.[2] Knee pain is a common clinical manifestation and can be associated with trauma or pathological fracture. Surgery can be offered if no other evidence of metastasis is seen elsewhere. However, bony metastasis from renal cell carcinoma appears to behave similarly to primary bone disease. Some experts believe there is no survival advantage by performing a wide resection in place of intralesional curettage and local stabilization.[2] The use of radiotherapy and bisphosphonates has also been advocated.
Conflicts of Interest
None declared.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published, and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
References
- Broomfield J, Ralte P, Morapudi S, Vasireddy N, Kershaw S.?Anterior knee pain: an unusual presentation of renal cell carcinoma. J Surg Case Rep 2014; 2014 (03) rju018
- Li G, Shan C, Sun R. et al.?Patellar metastasis from primary tumor. Oncol Lett 2018; 15 (02) 1389-1396
Address for correspondence
Publication History
Publication Date:
10
December 2021 (online)
? 2021. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd
Floor, Sector 2, Noida-201301 UP, India
|?Fig. 1X-ray skyline view showing a lytic lesion in the patella.
|?Fig. 2X-ray lateral view showing lesion filled with bone cement.
References
- , Ralte P, Morapudi S, Vasireddy N, Kershaw S.?Anterior knee pain: an unusual presentation of renal cell carcinoma. J Surg Case Rep 2014; 2014 (03) rju018
- Li G, Shan C, Sun R. et al.?Patellar metastasis from primary tumor. Oncol Lett 2018; 15 (02) 1389-1396