 PDF
PDF  Views
Views  Share
Share


Palliative Care in Oncology
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2020; 41(02): 215-217
DOI: DOI: 10.4103/ijmpo.ijmpo_27_20
The word palliative is derived from the Latin word ”pallium” meaning cloak. Palliative care is the active complete care of patients with life-limiting illnesses (not only cancer) and their families when the disease is not amenable to curative treatments. “Cloaking” or palliating a patient would involve tackling the psychological, social, and spiritual aspects of the disease and its treatment apart from the conventional care for physical symptom relief. Palliative care is a patient-centered approach that emphasizes relief from pain and distress by systematic identification and assessment of problems faced by the patient [Figure 1].[1]
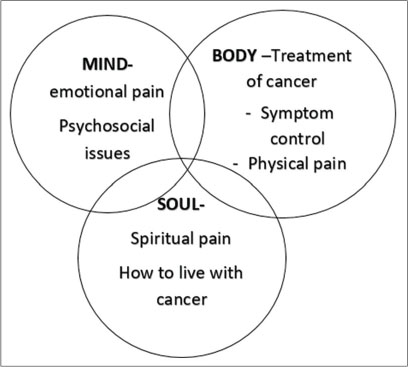
| Figure 1: Overview of palliative care. An integrated approach with the management of total pain – physical, emotional, spiritual, and social components[2]
In India, since 2012, we have had the National Program for Palliative Care, under the National Health Mission. There are also various initiatives by the government and the nongovernment organizations to tackle the increasing demand for palliative care services in the community. The community-based palliative care service in Kerala (Neighborhood Network in Palliative Care) is a model for resource-poor settings, where the people in the community are trained for providing basic palliative care services to the neighborhood patients. However, typically palliative care for cancer patients is delivered by multidisciplinary teams including clinical oncologists, palliative care physicians, physiotherapists, psychiatrists, dietitians, and palliative care nurses.[2]
In oncology, palliative care is extremely important at all stages of cancer care, as elaborated below [Figure 2].
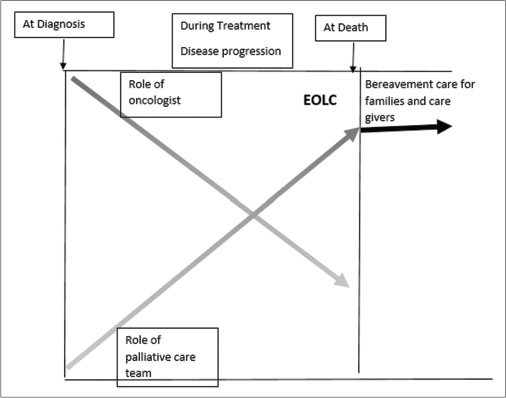
| Figure 2: Role of palliative care team throughout cancer treatment[2]
At diagnosisb
During treatment
End-of-life care (EOLC)
Publication History
Received: 27 January 2020
Accepted: 09 April 2020
Article published online:
23 May 2021
© 2020. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
The word palliative is derived from the Latin word ”pallium” meaning cloak. Palliative care is the active complete care of patients with life-limiting illnesses (not only cancer) and their families when the disease is not amenable to curative treatments. “Cloaking” or palliating a patient would involve tackling the psychological, social, and spiritual aspects of the disease and its treatment apart from the conventional care for physical symptom relief. Palliative care is a patient-centered approach that emphasizes relief from pain and distress by systematic identification and assessment of problems faced by the patient [Figure 1].[1]
| Figure 1: Overview of palliative care. An integrated approach with the management of total pain – physical, emotional, spiritual, and social components[2]
In India, since 2012, we have had the National Program for Palliative Care, under the National Health Mission. There are also various initiatives by the government and the nongovernment organizations to tackle the increasing demand for palliative care services in the community. The community-based palliative care service in Kerala (Neighborhood Network in Palliative Care) is a model for resource-poor settings, where the people in the community are trained for providing basic palliative care services to the neighborhood patients. However, typically palliative care for cancer patients is delivered by multidisciplinary teams including clinical oncologists, palliative care physicians, physiotherapists, psychiatrists, dietitians, and palliative care nurses.[2]
In oncology, palliative care is extremely important at all stages of cancer care, as elaborated below [Figure 2].
| Figure 2: Role of palliative care team throughout cancer treatment[2]
At diagnosisb
During treatment
End-of-life care (EOLC)
At Diagnosis
Breaking bad news
A six-step protocol called the SPIKES approach which included Setting up the session, evaluating the patients’ Perception, getting the patient’s Invitation, providing the necessary Knowledge, addressing the patient’s Emotions, and formulating a Strategy and summary is used to break the bad news to the patient.[3]
Integrating palliative care early into patient care has been proven to improve outcomes in some cancers. Early timely palliative care services in patients with lung cancer led to a better quality of life and mood as compared to standard care. These patients also had a more peaceful End of life care (EOLC) and longer survival.[4]
Symptom management
This applies to all stages of cancer care. The most important symptom is pain. Pain management is now a specialty by itself. The WHO ladder comprising step 1 (nonopioids), step 2 (weak opioids), and step 3 (strong opioids), with the option of addition of adjuvant drugs at each stage, is a very useful guide in the management of pain. We can follow the escalation or de-escalation approaches for analgesia based on the severity of pain.[5] The analgesics include NSAIDs, weak opioids, strong opioids, and adjuncts. The complications of the analgesics should also be managed by the same physician administering them. Analgesics are administered “by the mouth, by the clock and by the ladder.”
Newer developments in analgesia include newer drugs, easier delivery methods (transdermal patches of fentanyl and buprenorphine and oral transmucosal fentanyl citrate), patient-controlled analgesia, the use of interventional radiology or neurosurgical techniques (for neurolytic block therapy), and spinal stimulators to name a few.
During Treatment
Management of ongoing symptoms both disease-related and treatment-related such as pain, nausea, vomiting, anorexia, diarrhea, and neuropathy.
Although minor problems such as nausea, vomiting, and mild pain may be treated by the oncologist, symptoms such as intractable diarrhea, breathlessness, severe pain, and paresthesia related to neuropathy may require specialized care.
Psychosocial issues of patients
Patients have to deal with multiple stressors all of which take their toll on them, such as repeated investigations assessing the disease status, fertility issues, and financial stresses. Support from the palliative care and the psycho-oncology team is invaluable in such situations to help them cope well with the disease and treatment. This will also help in better compliance with treatment.
After Exhaustion of Curative Treatment Options and End-Of-Life Care
Management of treatment sequelae such as physical issues (like lymphedema) and social and economic issues due to cancer care
EOLC – To ensure that each patient has a “good” death.
EOLC
This includes the recognition of impending death, control of physical symptoms, fulfilling patient-centered needs, and above all safeguard the patient’s right to die in dignity, at a place of choice, and without unnatural and futile prolongation of life by medical means.[6]
EOLC is not limited to the last few hours or days of life but includes the stage of impending death: a period of around 6 months to 1 year before death.[7] This is a very stressful time for the family. Care given during this crucial period is remembered by the family for years to come.
Recognition of impending death
This step is important as it will help the medical team and the family to cope up with the ongoing process and complete the necessary formal/legal responsibilities of the patient. With good communication, the family will also be able to choose the further direction of care and take decisions such as place of EOLC (hospital vs. home), extent of investigations, means of nutrition support, hospital emergency visits, and plan spiritual rites. In cancer patients, it may be difficult to predict death accurately; however, clinical clues such as increasing weakness and disorientation, dry skin, decreased intake and output, weak pulse, cold skin, varying respiration patterns, and decreased speech may help in recognizing that death is imminent.[7]
Control of physical symptoms
Careful periodic review of all the medications is a vital part of EOLC. As the patient becomes weaker, it may be necessary to use alternative routes of delivery such as subcutaneous, sublingual, transdermal, or rectal and stop the unnecessary drugs. At this stage, it is important to provide anticipatory prescriptions with detailed instructions in the local language to the caregivers. Having emergency medications at hand and knowing what to do will enable the caregivers to provide immediate symptom relief to the patient without undue panic.
Furthermore, at this stage, the team should reassess the patient at frequent intervals to optimize the management of the patient and target new issues.
Pain – Analgesics are to be reviewed; for a hospitalized patient, a continuous infusion of morphine may be used.
Breathlessness – Low doses of morphine and small doses of sedatives such as lorazepam or midazolam to alleviate the associated anxiety help in this situation. The decision regarding oxygen use is to be individualized as per the patient, family, and the disease status of the patient.
Urinary problems – Catheters, adult diapers/pads, or bedpans can be used as per the convenience and choice of the patient and the family.
Nausea and vomiting need to be treated based on the cause.
Death rattle – This can be prevented by reducing the secretions with atropine or glycopyrronium bromide. Reassurance of the family is also important.
Agitation or restlessness can be treated with haloperidol or midazolam; however, reversible causes such as metabolic encephalopathy and dehydration also need to be considered and treated if possible.
Catastrophic events such as acute stridor, convulsions, and hemorrhage need to be anticipated and treatment options should be explained to the family to avoid undue emergency room visits.
The palliative care team plays an important role in coordinating between the physician and the family. Beyond symptom relief, they assist in reviewing the care protocols, stopping unnecessary medications/interventions, continuing communication, and providing psychosocial support by addressing ethical and spiritual issues of the patient and caregivers.[6]
In March 2018, The Supreme Court of India issued the directive for legal recognition of “advanced medical directives” or “living wills.” The treating doctor and the hospital should respect a patient’s decision regarding the withdrawal of life-saving treatment communicated in advance. This provision recognizes “the right to die with dignity” as a part of “Right to life”.[8]
Bereavement/grief counseling and care also provide a continuum of care for the family of the patients.
Although the guiding principles are similar, pediatric and geriatric patients need specialized palliative care. Thus, palliative care approach focuses on the quality of life of the patient and emphasizes on “adding life to years, rather than years to life.”
References
- Definition of Palliative Care. World Health Organization; 2002. Available from: http://www.who.int/cancer/palliative/definition/en. [Last accessed on 2020 Jan 20]
- Training Manual for Doctors and Nurses under National Programme for Palliative Care. The National Institute of Health and Family Welfare; Available from: https://dghs.gov.in/WriteReadData/userfiles/file/a/5127_1558685685054(1).pdf. [Last accessed on 2020 Jan 25].
- Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES – A six-step protocol for delivering bad news: Application to the patient with cancer. Oncologist 2000; 5: 302-11
- Temel JS, Greer JA, El-Jawahri A, Pirl WF, Park ER, Jackson VA. et al. Effects of early integrated palliative care in patients with lung and GI cancer: A randomized clinical trial. J Clin Oncol 2017; 35: 834-41
- WHO Pain Ladder. Available from: https://www.who.int/cancer/palliative/painladder/en/. [Last accessed on 2020 Jan 25]
- Macaden SC, Salins N, Muckaden M, Kulkarni P, Joad A, Nirabhawane V. et al. End of life care policy for the dying: Consensus position statement of Indian association of palliative care. Indian J Palliat Care 2014; 20: 171-81
- Indian Association of Palliative Care. Text book for Certificate Course in Essentials of Palliative Care. 5th ed. Jharkhand: IAPC; 2017
- Bandewar SV, Chaudhuri L, Duggal L, Nagral S. The supreme court of India on euthanasia: Too little, too late. Indian J Med Ethics 2018; 3: 91-4
Address for correspondence
Publication History
Received: 27 January 2020
Accepted: 09 April 2020
Article published online:
23 May 2021
© 2020. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
| Figure 1: Overview of palliative care. An integrated approach with the management of total pain – physical, emotional, spiritual, and social components[2]
| Figure 2: Role of palliative care team throughout cancer treatment[2]
References
- Definition of Palliative Care. World Health Organization; 2002. Available from: http://www.who.int/cancer/palliative/definition/en. [Last accessed on 2020 Jan 20]
- Training Manual for Doctors and Nurses under National Programme for Palliative Care. The National Institute of Health and Family Welfare; Available from: https://dghs.gov.in/WriteReadData/userfiles/file/a/5127_1558685685054(1).pdf. [Last accessed on 2020 Jan 25].
- Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES – A six-step protocol for delivering bad news: Application to the patient with cancer. Oncologist 2000; 5: 302-11
- Temel JS, Greer JA, El-Jawahri A, Pirl WF, Park ER, Jackson VA. et al. Effects of early integrated palliative care in patients with lung and GI cancer: A randomized clinical trial. J Clin Oncol 2017; 35: 834-41
- WHO Pain Ladder. Available from: https://www.who.int/cancer/palliative/painladder/en/. [Last accessed on 2020 Jan 25]
- Macaden SC, Salins N, Muckaden M, Kulkarni P, Joad A, Nirabhawane V. et al. End of life care policy for the dying: Consensus position statement of Indian association of palliative care. Indian J Palliat Care 2014; 20: 171-81
- Indian Association of Palliative Care. Text book for Certificate Course in Essentials of Palliative Care. 5th ed. Jharkhand: IAPC; 2017
- Bandewar SV, Chaudhuri L, Duggal L, Nagral S. The supreme court of India on euthanasia: Too little, too late. Indian J Med Ethics 2018; 3: 91-4