 PDF
PDF  Views
Views  Share
Share


Ovarian stromal tumor with minor sex cord elements with coexistent endometrial carcinoma
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2013; 34(01): 44-46
DOI: DOI: 10.4103/0971-5851.113432
Abstract
Ovarian stromal tumor with minor sex cord elements is a rare tumor. It is composed of predominantly fibrothecomatous tumor with scattered minor sex cord elements in less than 10% of the tumor area. These tumors may be hormonally active and predispose to carcinoma endometrium. A case of ovarian fibroma-thecoma with minor sex cord elements in which coexistent endometrial carcinoma was also discovered is being reported. Though thecoma may be a predisposing factor for endometrial cancer, meticulous histopathological examination of the ovary may reveal additional sources of estrogen like granulosa cell aggregates as in our patient. Such patients would require long-term follow-up to detect any recurrence of granulosa cell tumor.
Publication History
Article published online:
20 July 2021
© 2013. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Ovarian stromal tumor with minor sex cord elements is a rare tumor. It is composed of predominantly fibrothecomatous tumor with scattered minor sex cord elements in less than 10% of the tumor area. These tumors may be hormonally active and predispose to carcinoma endometrium. A case of ovarian fibroma–thecoma with minor sex cord elements in which coexistent endometrial carcinoma was also discovered is being reported. Though thecoma may be a predisposing factor for endometrial cancer, meticulous histopathological examination of the ovary may reveal additional sources of estrogen like granulosa cell aggregates as in our patient. Such patients would require long-term follow-up to detect any recurrence of granulosa cell tumor.
INTRODUCTION
Ovarian stromal tumor with minor sex cord elements was first described by Young and Scully in 1983.[1] Only 11 cases of ovarian stromal tumor with minor sex cord elements have been reported till date.[1,2,3,4,5,6,7] The increased estrogen production by these tumors is a risk factor for endometrial carcinoma. Only three cases of ovarian stromal tumors with minor sex cord elements with coexistent endometrial carcinoma have been reported.[1,8] We report a case of a 79-year-old female who presented with post-menopausal bleeding and an ovarian tumor which was post-operatively diagnosed as ovarian fibroma–thecoma with minor sex cord elements. Patient was also found to have well-differentiated endometrioid adenocarcinoma of uterus and underwent surgical staging for it.
CASE REPORT
A 79-year-old woman presented with post-menopausal bleeding and pain in lower abdomen for 2 months. The obstetric history of the patient was P2L2 and the patient had attained menopause 30 years back. The age of menarche was 14 years. On examination, a firm mass was palpable in lower abdomen extending upto umbilicus. On vaginal examination, uterus size could not be made out and a large abdomino pelvic mass was palpable. Abdominal ultrasonography revealed a normal-sized uterus with endometrial thickness of 7 mm and a 20 × 10 cm solid mass in pelvis and lower abdomen. Left ovary was not seen separately and there was minimal ascites. Patient underwent endometrial aspiration and it was reported as endometrioid adenocarcinoma (Grade 1). Patient underwent staging laparotomy which revealed a 20 × 10 cm solid left ovarian tumor. The right ovary was normal and there was minimal ascites which was sent for cytology. On exploration, intestines, liver and biliary tract, pancreas, omentum, and fallopian tubes were without lesions and the uterus was of normal size. The patient underwent total abdominal hysterectomy with bilateral salpingo-oophorectomy, infra-colic omentectomy, and pelvic lymphadenectomy and the specimen was submitted for histopathological examination.
Left ovary measured 21 × 14 × 10 cm and the cut section was homogenously fleshy with areas showing yellowish discoloration. Cut section of the uterus revealed a 4 × 3 cm exophytic fundal growth in the endometrial cavity infiltrating less than one-third of the myometrium. The right ovary, omentum, and bilateral fallopian tubes were grossly normal. On microscopic examination, left ovary showed features of a stromal tumor with minor sex cord elements [Figure 1]. The tumor comprised mainly of fibroma-thecoma component (more than 90%) with few aggregates of granulosa cells [Figure 2]. These granulosa cell aggregates were immunoreactive for inhibin [Figure 3a] and calretinin [Figure 3b].
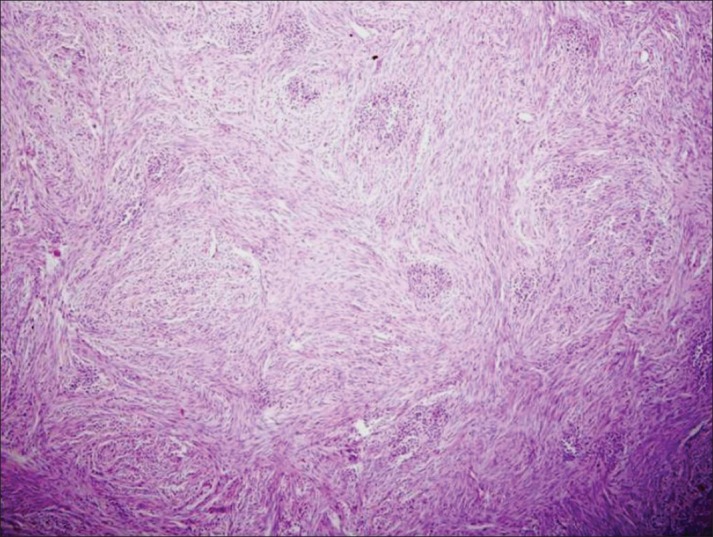
| Fig. 1 Stromal tumor with minor sex cord elements, fibroma with intermingled sex cord structures
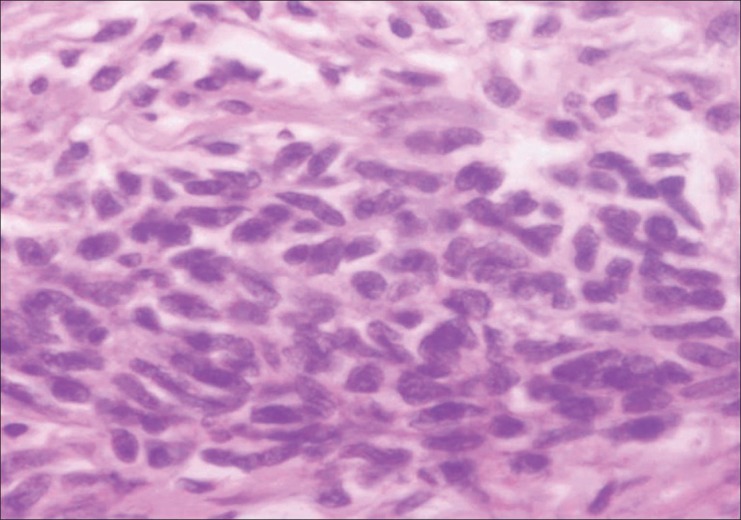
| Fig. 2 Sex cord structures show scant cytoplasm and a round to ovoid nucleus with a longitudinal groove resembling granulosa cells
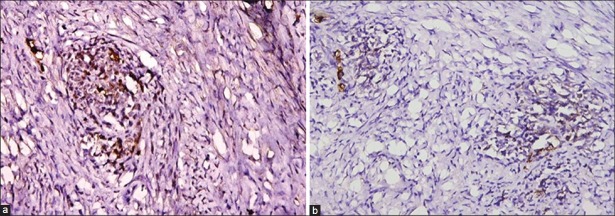
| Fig. 3 Granulosa cells showing positive immunostaining for (a) inhibin and (b) calretinin
Multiple sections from the endometrial growth showed features of a well-differentiated endometrioid adenocarcinoma (Grade I). The omentum and lymph nodes were free of tumor.
The patient did not receive radiotherapy post-operatively and she is on regular follow-up.
DISCUSSION
Ovarian fibromas with minor sex cord elements are rare tumors and only 11 such cases have been reported.[1,2,3,4,5,6,7] The predominant component in such tumors is generally fibroma or thecoma with sex cord elements dispersed randomly and occupy less than 10% of area of the total area of the tumor on any slide. The average age of presentation ranges from 16 to 65 years.[1] However, our patient was 79-year old. These patients usually present with bleeding per vaginum, pain abdomen, or abdominal mass. Our patient presented with bleeding per vaginum. The tumor size can range from 1 to 10 cm or ovary may be of normal size.[1,2] In our patient, the size of the tumor was 20 cm. The gross appearance of such tumors resembles fibroma or a thecoma, which are solid, firm, whitish-to-yellow neoplasm. On microscopy, they are composed of spindle-shaped cells, arranged in intersecting fascicles with variable amount of collagen and intermingled sex cord elements. Stromal cells have elongated nuclei with tapering ends and no prominent nucleoli. Sex cord components vary in appearance between fully differentiated granulosa cells and indifferent tubular structures resembling immature Sertoli cells.
Differential diagnoses include ovarian fibromatosis, Brenner tumor, and adenofibromas. In ovarian fibromatosis, there is a proliferation of spindle-shaped cells with abundant collagen formation and focal areas of edema. The normal follicular structures of the ovary are preserved in ovarian fibromatosis.[3,4] The epithelial aggregates of Brenner tumor are composed of transitional cells or mucinous cells. In adenofibroma, the glands are abundant, larger, and tubular and more variable in size when compared to uniform tubules of minor sex cord elements.[2]
In 1983, Young and Scully reported seven cases of fibromatous tumors of the ovary, of which five cases were ovarian fibroma with minor sex cord elements and the other two were luteinized thecoma and stromal-Leydig cell tumor with minor sex cord elements.[1] Two out of these seven cases also had well-differentiated adenocarcinoma in the endometrium. Zhang et al.[9] reported 50 cases of luteinized thecomas and stromal Leydig cell tumors. They found the presence of sex cord elements with granulosa cell morphology in only two of 50 cases. Lee et al.[8] reported a case of fibrothecoma with minor sex cord elements showing focal fibrosarcomatous change. The uterus showed multifocal endometrial adenocarcinoma of endometrioid type. A case of mucinous cystadenoma coexisting with stromal tumor with minor sex cord elements was reported by Yang et al.[10]
CONCLUSION
Ovarian stromal tumor with minor sex cord elements is a rare tumor, which may be hormonally active predisposing to carcinoma endometrium. Meticulous histopathological examination is essential for identification of the sex cord elements even if potential source of estrogen like the coma is present. Patients diagnosed with such tumors need regular follow-up as the clinical behavior and risk of recurrence in these patients require further evaluation.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
| Fig. 1 Stromal tumor with minor sex cord elements, fibroma with intermingled sex cord structures
| Fig. 2 Sex cord structures show scant cytoplasm and a round to ovoid nucleus with a longitudinal groove resembling granulosa cells
| Fig. 3 Granulosa cells showing positive immunostaining for (a) inhibin and (b) calretinin