 PDF
PDF  Views
Views  Share
Share


Outcome of CBV (Carmustine, Cyclophosphamide, Etoposide) Conditioning Regimen for Autologous Stem Cell Transplant in Lymphoma: A Retrospective Study from a Tertiary Cancer Center in South India
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2025; 46(01): 031-039
DOI: 10.1055/s-0041-1740134
Abstract
Introduction In autologous stem cell transplant (ASCT) for lymphomas, no standard conditioning regimen has been defined so far. Thus, the choice is guided by the center's familiarity and experience with a particular regimen.
Objective To determine the response, toxicity, and survival outcomes in lymphoma patients who underwent ASCT with CBV (cyclophosphamide, carmustine, and etoposide) conditioning regimen.
Materials and Methods Between January 2013 and May 2019, 45 consecutive lymphoma patients who had ASCT with CBV conditioning regimen were included in this retrospective study. CBV consisted of cyclophosphamide (1.5 g/m2/day × 4 days), carmustine (300 mg/m2 × 1 day), and etoposide (125 mg/m2 twice daily × 3 days). Baseline characteristics, pre transplant response, apheresis, post-transplant toxicities, post-transplant response, and survival outcomes were collected. Endpoints were toxicity, response, event-free survival (EFS), and overall survival (OS).
Results The median age was 30 (range: 6–64) years. Diagnosis was Hodgkin lymphoma (HL) in 26 (58%) and non-Hodgkin lymphoma (NHL) in 19 (42%). Forty-three patients (95%) had chemosensitive disease; 22(49%) in CR, and 21 (46%) in PR. The median CD34 was 2.95 × 106/kg (range: 0.9–9.56). The median time to neutrophil engraftment was 11 days (9–23) and 13 (8–36) days for platelets. All patients had febrile neutropenia, clinically and/or microbiologically documented infection was seen in 75%- of patients. The most common grade 3/4 toxicities were mucositis (n = 4, 9%), diarrhea (n = 4, 9%), and nausea/vomiting (n = 2, 4%). The average days of hospitalization was 18 (range: 10–37). Day 100 mortality was 6.6%- (n = 3). The median follow-up was 44.8 months. The median EFS for the entire cohort was 23.8 months; for HL, the median EFS was not reached, and for NHL, it was 7.97 months (95%- confidence interval [CI]: 1.57–14.37). The median OS for the entire cohort and for HL was not reached; for NHL, it was 24.3 months (95%- CI: 0.56–48.11).
Conclusion CBV conditioning regimen was well tolerated with low grade 3/4 toxicities and efficacy comparable to literature data.
Keywords
CBV conditioning regimen - autologous stem cell transplant - Hodgkin lymphoma - non-Hodgkin lymphomaAuthors' Contributions
Study conceptualization and methodology: SK, NK, BP, DK, CK, and BD. Data collection and analysis: NK, SK, BP, DK, CK, KR, and MR. Manuscript writing: NK, BP, SK, and PG. Review and editing: SK, BD, and PG. Final approval of manuscript: all authors.
Publication History
Article published online:
02 February 2022
© 2022. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
- Preemptive and Upfront Plerixafor: Safe and Effective Strategy for Patients Undergoing Autologous Stem Cell transplant and at High Risk for Mobilization FailureVipul Sheth, Indian Journal of Medical and Paediatric Oncology, 2020
- Analysis of Relapsed/Refractory Hodgkin Lymphoma Treated with Autologous Transplantation: A Single-Center ExperienceVishal Kulkarni, Indian Journal of Medical and Paediatric Oncology, 2020
- Adult Burkitt lymphoma: An institutional experience with a uniform chemotherapy protocolMukesh Patekar, South Asian Journal of Cancer, 2018
- Combined Modality Treatment with “Dexamethasone, Methotrexate, Ifosfamide, L-Asparaginase, and Etoposide ” Chemotherapy and Involved Field Radiotherapy for Earl...Vineet G Gupta, Indian Journal of Medical and Paediatric Oncology, 2018
- A Randomized, Multiple-Dose, Multicenter, Comparative Parallel Study to Evaluate the Safety and Efficacy of Intravenous Infusion of Rituximab (Hetero) and Refer...Suresh Advani, Indian Journal of Medical and Paediatric Oncology, 2018
- Significance of an intensified myeloablative conditioning regimen for myeloid malignancy and acute lymphoblastic leukemiaTadakazu Kondo, Medical*Online-E, 2018
- Efficacy and Safety of Intermediate dose Etoposide for Mobilization of Peripheral Blood Stem Cells in Hematopoietic TumorsTakuma Ishizaki, Medical*Online-E, 2018
- Treatment advances and prognosis for patients with adult T-cell leukemia-lymphomaHiroo Katsuya, Medical*Online-E, 2017
- Posttransplantation cyclosporine-induced lymphoproliferative disorders: clinical and radiologic manifestations.K M Harris, Radiology, 1987
- A single institutional retrospective evaluation for younger patients with primary central nervous lymphomas on a modified R-MPV regimen followed by radiotherapy...Keiichiro Hattori, Medical*Online-E, 2017
Abstract
Introduction In autologous stem cell transplant (ASCT) for lymphomas, no standard conditioning regimen has been defined so far. Thus, the choice is guided by the center's familiarity and experience with a particular regimen.
Objective To determine the response, toxicity, and survival outcomes in lymphoma patients who underwent ASCT with CBV (cyclophosphamide, carmustine, and etoposide) conditioning regimen.
Materials and Methods Between January 2013 and May 2019, 45 consecutive lymphoma patients who had ASCT with CBV conditioning regimen were included in this retrospective study. CBV consisted of cyclophosphamide (1.5 g/m2/day × 4 days), carmustine (300 mg/m2 × 1 day), and etoposide (125 mg/m2 twice daily × 3 days). Baseline characteristics, pre transplant response, apheresis, post-transplant toxicities, post-transplant response, and survival outcomes were collected. Endpoints were toxicity, response, event-free survival (EFS), and overall survival (OS).
Results The median age was 30 (range: 6–64) years. Diagnosis was Hodgkin lymphoma (HL) in 26 (58%) and non-Hodgkin lymphoma (NHL) in 19 (42%). Forty-three patients (95%) had chemosensitive disease; 22(49%) in CR, and 21 (46%) in PR. The median CD34 was 2.95 × 106/kg (range: 0.9–9.56). The median time to neutrophil engraftment was 11 days (9–23) and 13 (8–36) days for platelets. All patients had febrile neutropenia, clinically and/or microbiologically documented infection was seen in 75%- of patients. The most common grade 3/4 toxicities were mucositis (n = 4, 9%), diarrhea (n = 4, 9%), and nausea/vomiting (n = 2, 4%). The average days of hospitalization was 18 (range: 10–37). Day 100 mortality was 6.6%- (n = 3). The median follow-up was 44.8 months. The median EFS for the entire cohort was 23.8 months; for HL, the median EFS was not reached, and for NHL, it was 7.97 months (95%- confidence interval [CI]: 1.57–14.37). The median OS for the entire cohort and for HL was not reached; for NHL, it was 24.3 months (95%- CI: 0.56–48.11).
Conclusion CBV conditioning regimen was well tolerated with low grade 3/4 toxicities and efficacy comparable to literature data.
Keywords
CBV conditioning regimen - autologous stem cell transplant - Hodgkin lymphoma - non-Hodgkin lymphomaIntroduction
High-dose chemotherapy (HDC) followed by autologous stem cell transplant (ASCT) is the current standard of care for relapsed/refractory lymphoma.[1] [2] Several HDC regimens with varying drug combinations, with or without total body irradiation (TBI), have been in use as the conditioning protocol in autologous transplant of lymphomas. Most have shown similar efficacy but different toxicity profiles. Compared to chemotherapy-TBI regimens, chemotherapy-only regimens have demonstrated superiority in terms of disease-free survival (DFS), overall survival (OS), and lesser toxicity.[3] [4] Commonly used HDC regimens in ASCT for lymphoma include BEAM (BCNU, etoposide, cytarabine, and melphalan), BEAC (BCNU, etoposide, cytarabine, and cyclophosphamide), CBV (cyclophosphamide, BCNU, and etoposide), and LACE (lomustine, etoposide, cytarabine, and cyclophosphamide),[5] [6] [7] [8] [9] but no prospective randomized study has been done so far comparing these regimens. Most of the retrospective studies comparing various HDC regimens have shown variability in toxicity, and some have reported differences in disease outcomes.[3] [10] [11] [12] [13] [14] [15] [16]
In our center, CBV has been the commonest conditioning regimen used for autologous transplant in lymphomas. Unfortunately, data regarding the use of CBV are scant in contemporary published literature, and there are no reports on the use of CBV conditioning from India. This study has retrospectively analyzed the toxicity profile, engraftment kinetics, and survival outcomes of lymphoma patients who have undergone ASCT using a CBV conditioning regimen.
Methodology
Patient Population
From January 2013 to May 2019, all consecutive histology-proven relapsed or refractory Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL) patients, who had a complete or partial response to salvage chemotherapy and underwent ASCT at our center, with CBV conditioning regimen were included in this retrospective study. Patients who received other conditioning regimen were excluded from the study.
We collected the data for baseline characteristics, pre-transplant response, apheresis, post-transplant toxicities, post-transplant response, and survival outcomes from medical records maintained in the department. Endpoints were toxicity, post-transplant response, event-free survival (EFS), and overall survival (OS).
Pre-Transplant Assessment
Relapsed or refractory lymphoma was treated with 3 to 4 cycles of first- or second-line salvage chemotherapy depending on their primary diagnosis and previous treatment history. Post salvage response assessment was done with either contrast-enhanced computed tomography (CECT) scan or positron emission tomography and computed tomography (PET-CT) scan. Pre-transplant chemosensitivity was defined as either complete or partial response following salvage therapy. Evaluation was done for organ functions (renal, hepatic, cardiac, and pulmonary) and general fitness as per the department protocol for all patients prior to transplant.
Stem Cell Mobilization, Collection, and Cryopreservation
Peripheral blood (PB) stem cell mobilization was done with GCSF 5 µg/kg twice daily for 4 days. One day prior to apheresis, on the fourth day of mobilization, PB CD34 enumeration was done. Plerixafor was used 12 hours before apheresis if the PB CD34 was <20 xss=removed>3 or as per physician's discretion based on the baseline risk factors for poor mobilization. All patients had undergone peripheral blood stem cell (PBSC) harvest by apheresis, and stem cell enumeration was done at the end of harvest. PBSC collected were volume depleted and cryopreserved using 10%- of dimethyl sulfoxide (DMSO) and autologous plasma at –80°C until day 0 (day of stem cell reinfusion).
Conditioning Regimen
CBV conditioning regimen was given over a period of 6 days in the following schedule: BCNU (carmustine) 300 mg/m2 intravenous (iv) over 2 hours on D-6, cyclophosphamide 1.5 g/m2/day i.v. over 2 hours on D-6 to D-3, mesna 120%- of cyclophosphamide dose as i.v. infusion over 24 hours on D-6 to D-3, and 40%- of cyclophosphamide dose as i.v. infusion over 12 hours on D-2, etoposide 125 mg/m2/dose i.v. over 1 hour 12th hourly on D-6 to D-4. The above CBV schedule is considered as CBV (low) compared to the older regimen CBV (high), which used carmustine at 600 mg/m2.[10] [11]
Supportive Care
All patients received G-CSF 5 µg/kg/day subcutaneous (s.c.) starting on day +1 after stem cell infusion until the absolute neutrophil count (ANC) was greater than 0.5 × 109/L for least 3 days.[17] [18] Irradiated packed red cell concentrates and platelet concentrates were given to keep hemoglobin >8.0 g/dL and platelet count >20 × 109/L, respectively. Oral fluconazole and acyclovir were started from day 1 as antifungal and antiviral prophylaxis, respectively. Routine antibacterial prophylaxis was not given. Total parenteral nutrition (TPN) was administered in patients who developed grade 3–4 mucositis and in any grade mucositis with decreased food intake. Febrile neutropenia was managed as per the department antibiotic policy.
Study Definitions
Time to neutrophil engraftment was defined as the first of three consecutive days with an absolute neutrophil count of ≥ 0.5 × 109/L.[19] [20] Time to platelet engraftment was defined as the first of three consecutive days when the platelet count was maintained ≥ 20 × 109/L without platelet transfusion.[19] Engraftment syndrome was defined by the presence of noninfectious fever and one other symptom (i.e., skin involvement, diarrhea, or pulmonary manifestations) during the peri-engraftment period.[21] Regimen-related organ toxicities, evaluated in the first 100 days, were graded using the Seattle criteria, whereas mucositis and chemotherapy-induced nausea and vomiting (CINV) were graded using the National Cancer Institute Common Terminology Criteria For Adverse Events (NCI CTCAE) v4.0.[22] [23] The length of hospital stay (LOS) was defined as the time from the day of infusion of stem cell product (Day 0) to the day of hospital discharge. Transplant-related mortality (TRM) was defined as any death not related to relapse or disease progression during the first 100 days after the transplant. EFS (event-free survival) was defined as the time interval from the date of the transplant to disease progression, relapse, or death due to any cause. Overall survival (OS) was defined as the time from transplant to death due to any cause or date of the last follow-up.
Statistical Analysis
Descriptive statistics were used to summarize baseline disease features, pre-transplant disease status, patient characteristics, and post-transplant outcomes. Estimation of EFS and OS was done using the Kaplan–Meier method and compared using log rank test. Data were censored on 31 March 2020 for survival analysis. IBM SPSS Statistics for Windows, Version 19.0. Armonk, NY: IBM was used for analysis.
Ethics
The procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1964, as revised in 2013. The study was approved by the Institute Ethics committee (no. JIP/IEC/2016/30/979, dated 23.10.2016), and waiver of informed patient consent was granted.
Results
Baseline Characteristics and Pre-Transplant Data
During the study period, 45 patients (28 males and 17 females) underwent autologous transplant with a CBV conditioning regimen for refractory/relapsed lymphoma. The median age was 30 years (range: 6–64). Diagnosis was HL in 26 patients (58%) and NHL in 19 patients (42%). Of the 45 patients, 28 (62%) had relapsed after their primary treatment, and 15 (35%) had refractory disease. The median time from diagnosis to transplant was 19 months, and median lines of previous therapy were two. As a part of pretransplant response assessment, PET CT and CECT was done in 22 (49%) and 23 (51%) patients, respectively. Among the 45 patients, 43 (96%) had chemosensitive disease (either complete response [CR] or partial response [PR]). All patients had ECOG (Eastern Cooperative Oncology Group) performance status of 1 before transplant baseline clinical characteristics, and pre-transplant disease status is shown in [Table 1].
|
Features |
Entire Cohort (N = 45) |
HL (N = 26) |
NHL (N = 19) |
|
|---|---|---|---|---|
|
Age (at transplant) in years |
30 (6–64 years) |
26 (6–47) |
38 (19–64) |
|
|
Gender Male Female |
28 (62.2%) 17 (37.8%) |
17 (65%) 9 (35%) |
11 (58%) 8 (42%) |
|
|
Diagnosis (lymphoma) |
26 (58%) |
19 (42%) |
||
|
Relapsed |
28 (62%) |
14 (54%) |
14 (74%) |
|
|
Refractory |
15 (34%) |
12 (46%) |
3 (16%) |
|
|
Upfront (in CR1 for HR) |
2 (4%) |
– |
2 (10%) |
|
|
NHL |
Relapsed/refractory DLBCL |
– |
– |
12 (63%) |
|
ALCL (ALK negative) (upfront) |
2 (11%) |
|||
|
Relapsed FL |
2 (11%) |
|||
|
Relapsed PTCL |
1 (5%) |
|||
|
Relapsed AITL |
1 (5%) |
|||
|
Relapsed ALCL |
1 (5%) |
|||
|
Time from diagnosis to transplant in months (median, range) |
19 (5-102) |
21 (8–84) |
16 (5–102) |
|
|
Number of lines of treatment (median, range) |
2 (1–4) |
2 (1–4) |
2 (1–3) |
|
|
ECOG PS (median, range) |
1 (0–1) |
1 (0–1) |
1 (0–1) |
|
|
Chemosensitivity |
||||
|
Yes |
43 (95.6%) |
24 (92%) |
19 (100%) |
|
|
No |
2 (4.4%) |
2 (8%) |
0 |
|
|
Pre-transplant imaging for disease status PET CT-22 (49%) CECT–23 (51%) |
||||
|
PET CT response (N = 22) |
||||
|
CR (complete response) |
15 (68%) |
10 (77%) |
5 (55%) |
|
|
PR (partial response) |
7 (32%) |
3 (23%) |
4 (45%) |
|
|
SD (stable disease) |
0 |
0 |
0 |
|
|
PD (progressive disease) |
0 |
0 |
0 |
|
|
CECT response (N = 23) |
||||
|
CR (complete response) |
8 (35%) |
5 (39%) |
3 (30%) |
|
|
PR (partial response) |
13 (56%) |
6 (46%) |
7 (70%) |
|
|
SD (stable disease) |
1 (4.5) |
1 (7.5%) |
0 |
|
|
PD (progressive disease) |
1 (4.5%) |
1 (7.5%) |
0 |
|
|
Entire cohort (N = 45) |
HL (N = 26) |
NHL (N = 19) |
||
|---|---|---|---|---|
|
Day of engraftment |
Neutrophils |
11 (9–23) |
11 (9–17) |
10.5 (9–23) |
|
Platelets |
13 (8–36) |
12.50 (8–36) |
14.5 (11–30) |
|
|
Febrile neutropenia |
FUO |
11 (24%) |
8 (31%) |
3 (16%) |
|
CDI |
18 (40%) |
9 (35%) |
9 (47%) |
|
|
MDI |
10 (22%) |
5 (19%) |
5 (26%) |
|
|
CDI and MDI |
6 (14%) |
4 (15%) |
2 (11%) |
|
|
No of antibiotics |
4 (1–8) |
4 (2–8) |
4 (1–7) |
|
|
Organism |
Sterile |
26 (58%) |
15 (58%) |
11 (58%) |
|
Gram negative |
13 (30%) |
6 (23%) |
7 (37%) |
|
|
Gram positive |
0 |
0 |
0 |
|
|
Polymicrobial |
5 (10%) |
5 (19%) |
0 |
|
|
Fungal |
1 (2%) |
0 |
1 (5%) |
|
|
Mucositis |
Grade 0 |
10 (22%) |
3 (10%) |
7 (37%) |
|
Grade1–2 |
31 (69%) |
19 (76%) |
12 (63%) |
|
|
Grade 3–4 |
4 (9%) |
4 (14%) |
0 |
|
|
CINV |
Grade 0 |
9 (20%) |
4 (16%) |
5 (26%) |
|
Grade 1–2 |
34 (66%) |
20 (77%) |
14 (74%) |
|
|
Grade 3–4 |
2 (4%) |
2 (7%) |
0 |
|
|
Diarrhea |
Grade 0 |
21 (47%) |
13 (50%) |
8 (42%) |
|
Grade 1–2 |
20 (43%) |
10 (38%) |
10 (53%) |
|
|
Grade 3–4 |
4 (10%) |
3 (12%) |
1 (5%) |
|
|
TPN |
Yes |
4 (9%) |
4 (15%) |
– |
|
No |
41 (91%) |
22 (85%) |
19 (100%) |
|
|
Blood products |
PRBC |
3 (0–8) |
3 (0–8) |
3 (0–7) |
|
SDP |
4 (2–13) |
4 (2–12) |
4 (2–13) |
|
|
Length of stay in days (median, range) |
18 (10–37) |
25 (10–37) |
18 (10–30) |
|
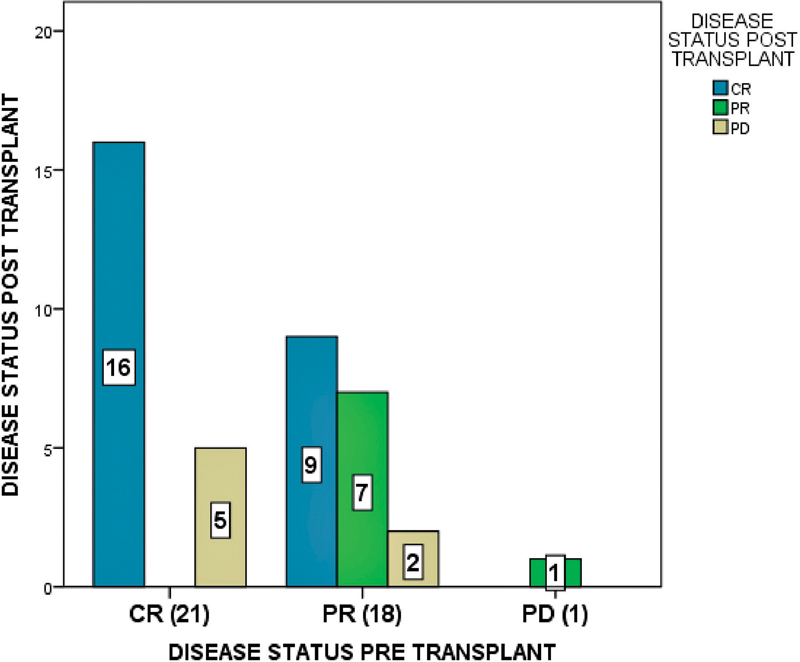
| Fig 1 Comparison of disease status pre and post-transplant in the entire cohort; CR, complete response, PR, partial response, PD, progressive disease. X axis indicates disease status pre-transplant and Y axis indicates disease status post-transplant. Among 21 patients who had CR pre transplant, 16 maintained CR, and 5 had progressive disease post-transplant. Among the 18 patients who had PR before transplant, 9 achieved CR, 7 maintained PR, and 2 had progressive disease. One patient who had progressive disease pre transplant achieved PR post-transplant.|
Survival
The median follow-up for the entire cohort was 44.8 months (95%- CI: 33.8–55.8). The median EFS for the entire cohort was 23.8 months (95%CI: 0.00–63.68); for HL, the median EFS was not reached, and for NHL, it was 7.97 months (95%CI: 1.57–14.37). Estimated 3-year EFS was 48% for the entire cohort; for HL and NHL, it was 57.4%- and 33.7%, respectively. The median OS for the entire cohort and for HL was not reached; for NHL, it was 24.3 months (95%CI: 0.56–48.11). The estimated OS at 3 years was 61.6%- for the entire cohort and 74.6%- and 43.4%- for HL and NHL, respectively.
An association of survival outcomes with respect to baseline features viz. relapsed vs. refractory disease, number of lines of salvage therapy, and pre-transplant disease status, complete response vs. partial response is shown in [Supplementary Tables S1] and [S2]. A comparison of survival outcomes based on the pre-transplant disease status of CR vs. PR in subgroups of HL and NHL, respectively, is shown in [Fig. 2].
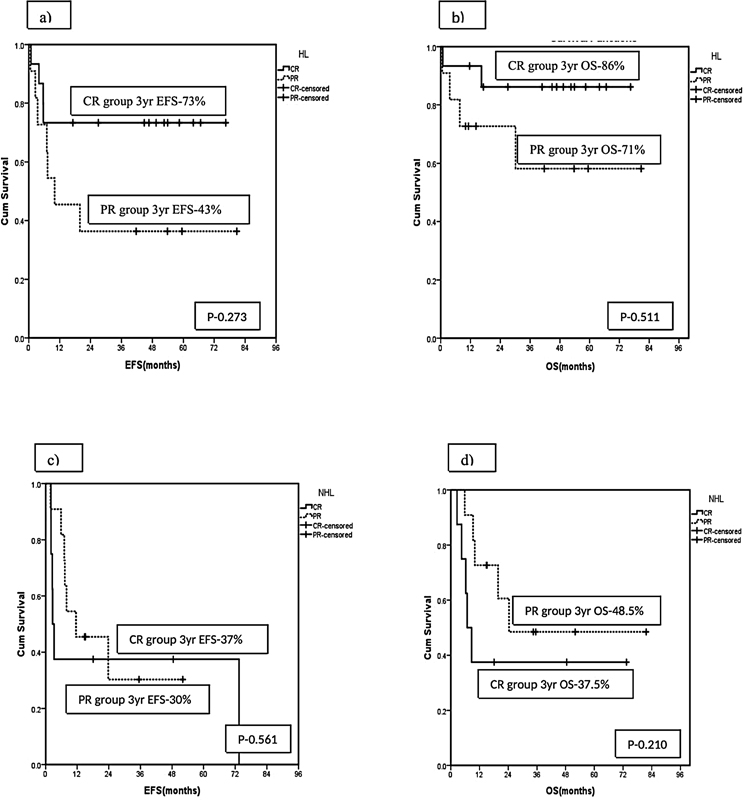
| Fig 2 Kaplan–Meier survival estimate for (A) event-free survival, (B) overall survival for Hodgkin lymphoma, and (C) event-free survival (D) overall survival for non-Hodgkin lymphoma, comparing outcomes with respect to pre-transplant disease status.|
Discussion
The present standard of care for relapsed/refractory lymphoma is HDC followed by ASCT.[2] [5] Several HDC regimens have been in use as conditioning protocol in the autologous transplant of lymphomas, and most have shown similar efficacy but with different toxicity profiles. CBV is one of the older conditioning regimens for lymphoma with a relatively safer toxicity profile, especially with low-dose CBV. Sparse data are available on the contemporary use of CBV, especially from India. Our study found CBV practicable, less toxic, and had efficacy comparable to that reported in the literature for other regimens used in lymphoma conditioning.
We report the results of 45 transplants for HL and NHL with CBV conditioning. The majority of the patients (95%) had chemosensitive disease at transplant. Grade 3 or 4 toxicities were observed in only 10%- of our patients, common toxicities being mucositis, diarrhea, and CINV. No grade 3/4 toxicity was observed in other organs viz. renal, liver, pulmonary, or cardiac. Toxicity in our study was comparable to that reported for low-dose CBV.[10] [11] [16] Studies with the original CBV (high dose) regimen with BCNU dose of 600 mg/m2 have reported higher pulmonary toxicity (5–10%). However, subsequent reports with the use of BCNU at 450 mg/m2 or 300 mg/m2 (CBV low) have shown less pulmonary toxicity (<1 href="https://www.thieme-connect.com/products/ejournals/html/10.1055/s-0041-1740134#JR212340337-10" xss=removed>10] [11] [12] [16] Also, Chen et al proved that carmustine dose higher than 300 mg/m2 resulted only in increased toxicity without any survival benefit.[10] Other grade 3 or 4 toxicities with CBV (low) included mucositis in about 8 to 25%, diarrhea 10 to 25%, CINV 4 to 8%- from various studies in the literature.[10] [14] [16] As summarized in [Table 3], grade 3/4 regimen-related toxicities were relatively less with CBV (low) compared to other commonly used conditioning regimens such as BEAM, BEAC, or LACE (10–25%- in CBV low vs. 30–55%- in other regimens) although with comparable survival outcomes.
|
Study |
Regimen |
Toxicity |
TRM (d100-150) |
PFS |
OS |
|---|---|---|---|---|---|
|
Arranz et al 1997, Spain[11] HL (n = 49) Retrospective study |
CBVhigh vs. CBVlow |
Not reported |
9%- vs. 8%- |
47%- vs. 29%- (p = 0.57) |
Not reported |
|
Salar et al, 2001, Spain[3] NHL (n = 395) Retrospective study |
CBV vs. BEAM vs. CyTBI |
Not reported |
Not reported |
CBV vs. BEAM Relative risk 1.26 (0.77–2.05) (p = 0.34) |
CBV vs. BEAM Relative risk 1.30 (0.74–2.28) (p = 0.36) |
|
Puig et al, 2005, Spain[12] (n = 113) NHL(n = 69) HL (n = 44) Retrospective study |
CBVhigh vs. BEAM |
Mucositis (grade 1–2) 6%- vs. 34%- Pulmonary (grade 3) 4%- vs. 0%- SOS: 5%vs. 0%- |
24%- vs. 5%- |
Not reported |
Not reported |
|
Harris et al, COG A5962, 2011, USA[16] HL (n = 28) NHL (n = 10) Prospective study |
CBV single arm study CBVhigh:450mg/m2 CBVlow:300mg/m2 |
CBVhigh vs. CBVlow Pulmonary toxicity (grade 3/4) 100%vs. 0% |
Not reported |
3year EFS HL:45%- NHL:30%- |
3year OS HL:63%- NHL:34%- |
|
Sharma et al, 2013 , India[15] (n = 51) NHL (n = 26) HL (n = 25) Retrospective study |
BEAM vs. LEAM |
Mucositis (grade 3/4) 68%vs. 65%- Diarrhea (grade 3/4) 47%vs. 41%- |
18%vs. 12%- |
2 year EFS (HL + NHL) 44.6%vs. 41.1%(p = 0.510) |
2 year OS (HL + NHL) 61.7%vs. 62.7%- (p = 0.928) |
|
Chen et al, 2015, Multicenter study[10] (n = 4,917) NHL (n = 3,905) HL (n = 1,012) Retrospective study |
CBVhigh vs. CBVlow vs. BEAM vs. BuCy vs. TBI |
CBVhigh vs. CBVlow vs. BEAM Overall toxicity (grade 3–4) 6%vs. 3%vs. 3%- |
Not reported |
CBVhigh vs. CBVlow vs. BEAM 3 year PFS HL 57%vs. 60%vs. 62%- DLBCL 39%vs. 47%vs. 47%- |
CBVhigh vs. CBVlow vs. BEAM 3 year OS HL 68%vs. 73%vs. 78%- DLBCL 43%vs. 55%vs. 58%- |
|
Khattry et al 2016, India[13] (N = 139) NHL = 92 HL = 47 Retrospective study |
LACE vs. BEAM |
Mucositis (grade 3–4) 8%vs. 38%- |
9%vs. 13%- |
5-year PFS HL: 39%vs. 48%- (p = 0.747) NHL: 34%vs. 46%- (p = 0.709) |
5-year OS HL: 49%vs. 48%- p = 0.279 NHL 37%vs. 46%- (p = 0.709) |
|
SHI et al 2016, China[14] NHL (n = 129) Retrospective study |
CBV vs. BEAM vs. BEAC |
CBV vs. BEAM Diarrhea(≥ grade 2) 18.8%vs. 63.9%- Mucositis (≥grade 2) 25%vs. 47.2%- |
0%- |
CBV vs. BEAM vs. BEAC 5-year EFS 43.8%vs. 66.7%vs. 67.5%- (p = 0.40) |
CBV vs. BEAM vs. BEAC 5-year OS 68.8%vs. 77.8%vs. 81.8%- (p = 0.584). |
|
Our study (N = 45) HL = 26 NHL = 19 Retrospective study |
CBV–single arm |
Diarrhea (grade 3/4) 10%. Mucositis (grade 3/4) 9%. |
6.6%. |
3-year EFS HL 57.4%. NHL 33.7%. |
3-year OS HL 74.6%. NHL 43.4%. |
References
- Philip T, Biron P. High-dose chemotherapy and autologous bone marrow transplantation in diffuse intermediate- and high-grade non-Hodgkin lymphoma. Crit Rev Oncol Hematol 2002; 41 (02) 213-223
- Sureda A, Bader P, Cesaro S. et al. Indications for allo- and auto-SCT for haematological diseases, solid tumours and immune disorders: current practice in Europe, 2015. Bone Marrow Transplant 2015; 50 (08) 1037-1056
- Salar A, Sierra J, Gandarillas M. et al; GEL/TAMO Spanish Cooperative Group. Autologous stem cell transplantation for clinically aggressive non-Hodgkin's lymphoma: the role of preparative regimens. Bone Marrow Transplant 2001; 27 (04) 405-412
- Mounier N, Gisselbrecht C. Conditioning regimens before transplantation in patients with aggressive non-Hodgkin's lymphoma. Ann Oncol 1998; 9 (Suppl. 01) S15-S21
- Philip T, Guglielmi C, Hagenbeek A. et al. Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-Hodgkin's lymphoma. N Engl J Med 1995; 333 (23) 1540-1545
- Isidori A, Christofides A, Visani G. Novel regimens prior to autologous stem cell transplantation for the management of adults with relapsed/refractory non-Hodgkin lymphoma and Hodgkin lymphoma: alternatives to BEAM conditioning. Leuk Lymphoma 2016; 57 (11) 2499-2509
- Philip T, Chauvin F, Bron D. et al. PARMA international protocol: pilot study on 50 patients and preliminary analysis of the ongoing randomized study (62 patients). Ann Oncol 1991; 2 (Suppl. 01) 57-64
- Rajamanickam D, Gokarn A, Gupta A. et al. LACE - an effective conditioning regimen for lymphoma patients undergoing autologous transplant- analysis of outcomes and prognostic factors. J Cancer Res Ther 2018; 14 (05) 926-933
- Galieni P, Troiani E, Bigazzi C. et al. Modified BEAM as conditioning regimen for lymphoma patients undergoing autologous hematopoietic stem cell transplantation. Bone Marrow Transplant 2018; 53 (01) 91-93
- Chen Y-B, Lane AA, Logan B. et al. Impact of conditioning regimen on outcomes for patients with lymphoma undergoing high-dose therapy with autologous hematopoietic cell transplantation. Biol Blood Marrow Transplant 2015; 21 (06) 1046-1053
- Arranz R, Tomás JF, Gil-Fernández JJ. et al. Autologous stem cell transplantation (ASCT) for poor prognostic Hodgkin's disease (HD): comparative results with two CBV regimens and importance of disease status at transplant. Bone Marrow Transplant 1998; 21 (08) 779-786
- Puig N, de la Rubia J, Remigia MJ. et al. Morbidity and transplant-related mortality of CBV and BEAM preparative regimens for patients with lymphoid malignancies undergoing autologous stem-cell transplantation. Leuk Lymphoma 2006; 47 (08) 1488-1494
- Khattry N, Gupta A, Jain R. et al. LACE versus BEAM conditioning in relapsed and refractory lymphoma transplant: retrospective multicenter analysis of toxicity and efficacy. Int J Hematol 2016; 103 (03) 292-298
- Shi Y, Liu P, Zhou S. et al. Comparison of CBV, BEAM and BEAC high-dose chemotherapy followed by autologous hematopoietic stem cell transplantation in non-Hodgkin lymphoma: efficacy and toxicity. Asia Pac J Clin Oncol 2017; 13 (05) e423-e429
- Sharma A, Kayal S, Iqbal S, Malik PS, Raina V. Comparison of BEAM vs. LEAM regimen in autologous transplant for lymphoma at AIIMS. Springerplus 2013; 2: 489
- Harris RE, Termuhlen AM, Smith LM. et al. Autologous peripheral blood stem cell transplantation in children with refractory or relapsed lymphoma: results of Children's Oncology Group study A5962. Biol Blood Marrow Transplant 2011; 17 (02) 249-258
- Colby C, McAfee SL, Finkelstein DM, Spitzer TR. Early vs delayed administration of G-CSF following autologous peripheral blood stem cell transplantation. Bone Marrow Transplant 1998; 21 (10) 1005-1010
- de Azevedo AM, Nucci M, Maiolino A. et al. A randomized, multicenter study of G-CSF starting on day +1 vs day +5 after autologous peripheral blood progenitor cell transplantation. Bone Marrow Transplant 2002; 29 (09) 745-751
- Valcárcel D, Sureda A. Graft failure. In: Carreras E, Dufour C, Mohty M, Kröger N. eds. The EBMT Handbook: Hematopoietic Stem Cell Transplantation and Cellular Therapies. 7th ed.. Springer; 2019: 307-313
- Murray S. Engraftment. In: Maziarz RT, Slater SS. eds. Blood and Marrow Transplant Handbook: Comprehensive Guide for Patient Care. Springer International Publishing; 2015: 161-165
- Maiolino A, Biasoli I, Lima J, Portugal AC, Pulcheri W, Nucci M. Engraftment syndrome following autologous hematopoietic stem cell transplantation: definition of diagnostic criteria. Bone Marrow Transplant 2003; 31 (05) 393-397
- Bearman SI, Appelbaum FR, Buckner CD. et al. Regimen-related toxicity in patients undergoing bone marrow transplantation. J Clin Oncol 1988; 6 (10) 1562-1568
- Common Terminology Criteria for Adverse Events (CTCAE) | Protocol Development | CTEP. Accessed October 18, 2021 at: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm
- Dos Santos KB, Costa LJM, Bettarello G. et al. LEAM versus CBV for conditioning in autologous hematopoietic stem cell transplantation for lymphoma. Bone Marrow Transplant 2019; 54 (04) 625-628
- Bishop MR, Dean RM, Steinberg SM. et al. Correlation of pretransplant and early post-transplant response assessment with outcomes after reduced-intensity allogeneic hematopoietic stem cell transplantation for non-Hodgkin's lymphoma. Cancer 2010; 116 (04) 852-862
- Nieto Y, Popat U, Anderlini P. et al. Autologous stem cell transplantation for refractory or poor-risk relapsed Hodgkin's lymphoma: effect of the specific high-dose chemotherapy regimen on outcome. Biol Blood Marrow Transplant 2013; 19 (03) 410-417
| Fig 1 Comparison of disease status pre and post-transplant in the entire cohort; CR, complete response, PR, partial response, PD, progressive disease. X axis indicates disease status pre-transplant and Y axis indicates disease status post-transplant. Among 21 patients who had CR pre transplant, 16 maintained CR, and 5 had progressive disease post-transplant. Among the 18 patients who had PR before transplant, 9 achieved CR, 7 maintained PR, and 2 had progressive disease. One patient who had progressive disease pre transplant achieved PR post-transplant.|
| Fig 2 Kaplan–Meier survival estimate for (A) event-free survival, (B) overall survival for Hodgkin lymphoma, and (C) event-free survival (D) overall survival for non-Hodgkin lymphoma, comparing outcomes with respect to pre-transplant disease status.|
References
- Philip T, Biron P. High-dose chemotherapy and autologous bone marrow transplantation in diffuse intermediate- and high-grade non-Hodgkin lymphoma. Crit Rev Oncol Hematol 2002; 41 (02) 213-223
- Sureda A, Bader P, Cesaro S. et al. Indications for allo- and auto-SCT for haematological diseases, solid tumours and immune disorders: current practice in Europe, 2015. Bone Marrow Transplant 2015; 50 (08) 1037-1056
- Salar A, Sierra J, Gandarillas M. et al; GEL/TAMO Spanish Cooperative Group. Autologous stem cell transplantation for clinically aggressive non-Hodgkin's lymphoma: the role of preparative regimens. Bone Marrow Transplant 2001; 27 (04) 405-412
- Mounier N, Gisselbrecht C. Conditioning regimens before transplantation in patients with aggressive non-Hodgkin's lymphoma. Ann Oncol 1998; 9 (Suppl. 01) S15-S21
- Philip T, Guglielmi C, Hagenbeek A. et al. Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-Hodgkin's lymphoma. N Engl J Med 1995; 333 (23) 1540-1545
- Isidori A, Christofides A, Visani G. Novel regimens prior to autologous stem cell transplantation for the management of adults with relapsed/refractory non-Hodgkin lymphoma and Hodgkin lymphoma: alternatives to BEAM conditioning. Leuk Lymphoma 2016; 57 (11) 2499-2509
- Philip T, Chauvin F, Bron D. et al. PARMA international protocol: pilot study on 50 patients and preliminary analysis of the ongoing randomized study (62 patients). Ann Oncol 1991; 2 (Suppl. 01) 57-64
- Rajamanickam D, Gokarn A, Gupta A. et al. LACE - an effective conditioning regimen for lymphoma patients undergoing autologous transplant- analysis of outcomes and prognostic factors. J Cancer Res Ther 2018; 14 (05) 926-933
- Galieni P, Troiani E, Bigazzi C. et al. Modified BEAM as conditioning regimen for lymphoma patients undergoing autologous hematopoietic stem cell transplantation. Bone Marrow Transplant 2018; 53 (01) 91-93
- Chen Y-B, Lane AA, Logan B. et al. Impact of conditioning regimen on outcomes for patients with lymphoma undergoing high-dose therapy with autologous hematopoietic cell transplantation. Biol Blood Marrow Transplant 2015; 21 (06) 1046-1053
- Arranz R, Tomás JF, Gil-Fernández JJ. et al. Autologous stem cell transplantation (ASCT) for poor prognostic Hodgkin's disease (HD): comparative results with two CBV regimens and importance of disease status at transplant. Bone Marrow Transplant 1998; 21 (08) 779-786
- Puig N, de la Rubia J, Remigia MJ. et al. Morbidity and transplant-related mortality of CBV and BEAM preparative regimens for patients with lymphoid malignancies undergoing autologous stem-cell transplantation. Leuk Lymphoma 2006; 47 (08) 1488-1494
- Khattry N, Gupta A, Jain R. et al. LACE versus BEAM conditioning in relapsed and refractory lymphoma transplant: retrospective multicenter analysis of toxicity and efficacy. Int J Hematol 2016; 103 (03) 292-298
- Shi Y, Liu P, Zhou S. et al. Comparison of CBV, BEAM and BEAC high-dose chemotherapy followed by autologous hematopoietic stem cell transplantation in non-Hodgkin lymphoma: efficacy and toxicity. Asia Pac J Clin Oncol 2017; 13 (05) e423-e429
- Sharma A, Kayal S, Iqbal S, Malik PS, Raina V. Comparison of BEAM vs. LEAM regimen in autologous transplant for lymphoma at AIIMS. Springerplus 2013; 2: 489
- Harris RE, Termuhlen AM, Smith LM. et al. Autologous peripheral blood stem cell transplantation in children with refractory or relapsed lymphoma: results of Children's Oncology Group study A5962. Biol Blood Marrow Transplant 2011; 17 (02) 249-258
- Colby C, McAfee SL, Finkelstein DM, Spitzer TR. Early vs delayed administration of G-CSF following autologous peripheral blood stem cell transplantation. Bone Marrow Transplant 1998; 21 (10) 1005-1010
- de Azevedo AM, Nucci M, Maiolino A. et al. A randomized, multicenter study of G-CSF starting on day +1 vs day +5 after autologous peripheral blood progenitor cell transplantation. Bone Marrow Transplant 2002; 29 (09) 745-751
- Valcárcel D, Sureda A. Graft failure. In: Carreras E, Dufour C, Mohty M, Kröger N. eds. The EBMT Handbook: Hematopoietic Stem Cell Transplantation and Cellular Therapies. 7th ed.. Springer; 2019: 307-313
- Murray S. Engraftment. In: Maziarz RT, Slater SS. eds. Blood and Marrow Transplant Handbook: Comprehensive Guide for Patient Care. Springer International Publishing; 2015: 161-165
- Maiolino A, Biasoli I, Lima J, Portugal AC, Pulcheri W, Nucci M. Engraftment syndrome following autologous hematopoietic stem cell transplantation: definition of diagnostic criteria. Bone Marrow Transplant 2003; 31 (05) 393-397
- Bearman SI, Appelbaum FR, Buckner CD. et al. Regimen-related toxicity in patients undergoing bone marrow transplantation. J Clin Oncol 1988; 6 (10) 1562-1568
- Common Terminology Criteria for Adverse Events (CTCAE) | Protocol Development | CTEP. Accessed October 18, 2021 at: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm
- Dos Santos KB, Costa LJM, Bettarello G. et al. LEAM versus CBV for conditioning in autologous hematopoietic stem cell transplantation for lymphoma. Bone Marrow Transplant 2019; 54 (04) 625-628
- Bishop MR, Dean RM, Steinberg SM. et al. Correlation of pretransplant and early post-transplant response assessment with outcomes after reduced-intensity allogeneic hematopoietic stem cell transplantation for non-Hodgkin's lymphoma. Cancer 2010; 116 (04) 852-862
- Nieto Y, Popat U, Anderlini P. et al. Autologous stem cell transplantation for refractory or poor-risk relapsed Hodgkin's lymphoma: effect of the specific high-dose chemotherapy regimen on outcome. Biol Blood Marrow Transplant 2013; 19 (03) 410-417