 PDF
PDF  Views
Views  Share
Share


Multiple solitary extramedullary anaplastic plasmacytomas
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2016; 37(04): 303-304
DOI: DOI: 10.4103/0971-5851.195727

Publication History
Article published online:
12 July 2021
© 2016. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
A 41-year-old female homemaker presented with a sudden-onset nontraumatic pain, swelling, and redness in her left calf of 1-week duration. Clinical features were suggestive of cellulitis (or deep vein thrombosis, which was ruled out by venous Doppler). The patient responded to conservative management and was discharged after 1 week.
Three months later, she returned with the same clinical features and a posterior bulge in the calf. Magnetic resonance imaging (MRI) revealed a well-circumscribed (11.1 cm × 7.0 cm × 4.4 cm) lesion within the soleus muscle, suggestive of a sarcoma [Figure 1]. An incisional biopsy was performed. From histopathology and immunohistochemistry studies, it was diagnosed as anaplastic plasmacytoma [Figures [Figures22 and and3].3]. Serum calcium, total protein, electrophoresis, and bone marrow trephine and biopsy were all essentially normal. The skeletal survey did not reveal any lytic lesion. Contrast computed tomography (CT) of the abdomen and thorax revealed another well-defined (15.9 cm × 13.6 cm × 12.3 cm) soft tissue lesion in the retroperitoneum, suggestive of a lymphoid mass [Figure 4]. CT-guided biopsy revealed the same anaplastic features of plasmacytoma.
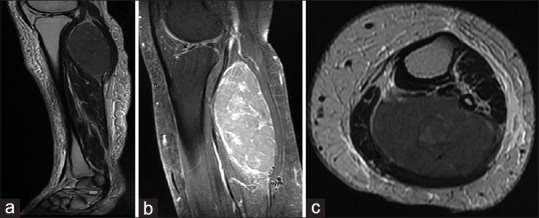
| Fig. 1 Magnetic resonance imaging of the leg: (a) Sagittal section T2-weighted image showing a well-defined mass with increased signal intensity confined within the soleus muscle; (b) sagittal section T1-weighted image with postcontrast enhancement-mass showing increased contrast enhancement; (c) axial T2-weighted image
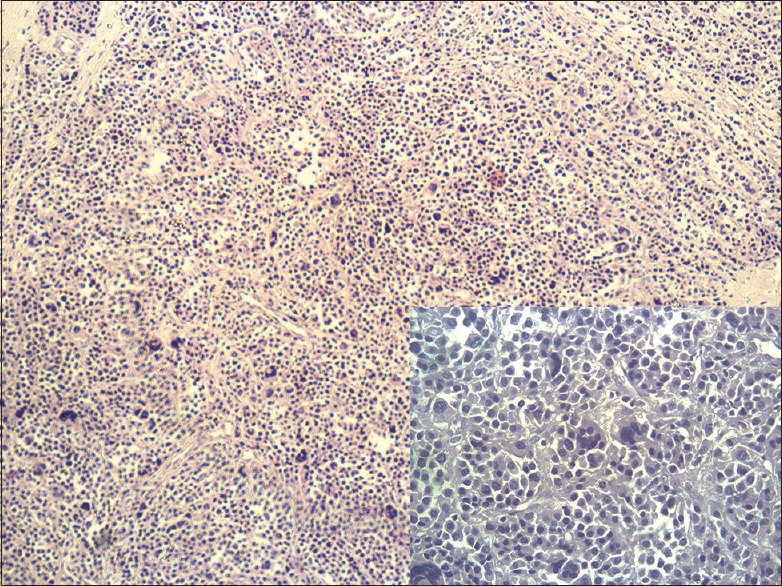
| Fig. 2 Section showing a tumor composed of solid sheets and nests of cells with round coarse nuclei and eosinophilic cytoplasm and plasma cells with intervening fibrous stroma showing hemorrhage (inlet: in high power field binucleated, multinucleated and bizarre cells with abundant mitotic figures are seen)
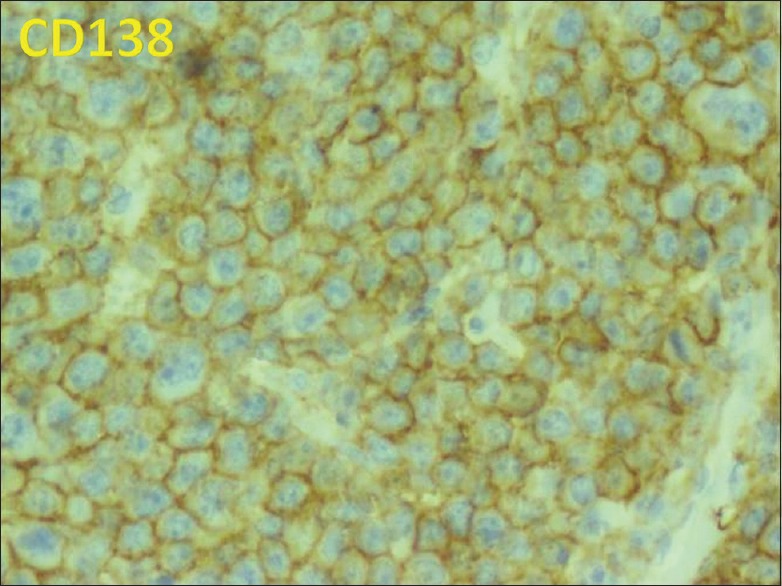
| Fig. 3 Tumor cells diffusely positive for CD138 (plasma cell associated antigen)
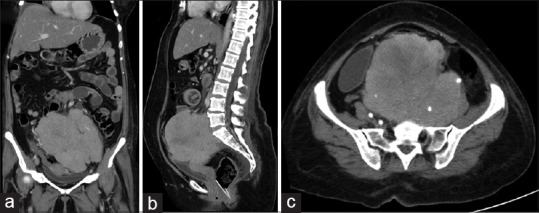
| Fig. 4 Contrast-enhanced computed tomography of the abdomen: (a) Coronal; (b) sagittal; (c) axial sections showing a large soft tissue attenuation retroperitoneal lesion with predominantly homogenous contrast enhancement extending from just below the level of aortic bifurcation till the left adnexal region below
In view of this retroperitoneal lesion, lenalidomide and dexamethasone combination chemotherapy was commenced. After four cycles, lenalidomide was replaced by bortezomib for another six more cycles. Serum electrophoresis performed during chemotherapy was found to be normal on several occasions. As she developed bilateral hydronephrosis due to compression and encasement of the ureters, external beam radiation therapy was initiated at 30 Gray (planned for 10 fractions). Unfortunately, the patient's general health rapidly deteriorated and she succumbed to renal failure and pneumonitis at the end of fifth fraction, 12 months from the time of first presentation.
Plasmacytoma is of two types: Solitary bone plasmacytoma and extramedullary plasmacytoma (EMP). EMPs make up 4% of all plasma cell tumors and occur mainly in the upper aerodigestive tract (UAD) (82.2%), with rare sites being retroperitoneum (1.3%) and musculature (0.6%).[1] In most of the instances, EMP is usually found solitary with conversion to multiple myeloma seen in about 14.1% in EMP arising from non-UAD areas.[1] In 2002, the International Myeloma Working Group recognized another distinct entity: Multiple solitary plasmacytomas (± recurrent) (MSPs) with lesions either extramedullary or osseous without any evidence of multiple myeloma (increased calcium, renal insufficiency, anemia, or bone lesions).[2] In the index case, two extremely rare sites (soleus muscle and the retroperitoneum) were involved at the time of presentation without any osseous involvement or end organ damage. When an extramedullary site involved is an extremity, it can masquerade as other common conditions such as cellulitis, deep vein thrombosis, abscess, or a ruptured baker's cyst. Other differential diagnosis for such intramuscular lesions to be considered includes sarcoma (as was suspected in the index case following MRI), granuloma, neurofibroma, lymphoma, and metastasis.[3] EMP is amenable to surgery/radiotherapy and has good prognosis; however, large numbers of solitary plasmacytomas or recurrent lesions at short intervals are an indication for systemic therapy.[2] High-grade anaplastic nature of the lesions, poor response to chemotherapy, extensive involvement of the retroperitoneum, and rapid progression eventually culminated into a fatal clinical course in the present case.
- This case highlights the clinical and radiological features of a rare plasma cell tumor – MSP involving two very unusual sites that were anaplastic in nature
- The occurrence of a plasmacytoma arising within the soleus muscle has not been previously reported the literature
- The primary presentation of an EMP arising in an extremity can be very deceptive
- The emphasis is to consider plasmacytoma as a differential diagnosis for intramuscular lesions as it mimics clinically and radiologically numerous common conditions of the lower limb that can eventually delay in appropriate diagnosis and management.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.