 PDF
PDF  Views
Views  Share
Share


Multidisciplinary Treatment of Pediatric Low-Grade Glioma: Experience of Children Cancer Hospital of Egypt; 2007-2012
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2018; 39(04): 488-492
DOI: DOI: 10.4103/ijmpo.ijmpo_79_17
Abstract
Background: Pediatric gliomas comprise a clinically, histologically, and molecularly heterogeneous group of central nervous system tumors. The survival of children with gliomas influenced by histologic subtype, age, and extent of resection. Tumor grade emerged as the most determinant of survival except in the young age groups. The aim of this study was to evaluate the role of multidisciplinary therapeutic approach including surgery and chemotherapy, and their impact on the outcome in pediatric patients with low-grade glioma (LGG). Procedure: Study patients were prospectively enrolled onto the study. All patients were below 18-year-old, diagnosed as LGG between July 2007 and June 2012. Upfront surgical resection was attempted in all tumors other than optic pathway sites. Systemic chemotherapy was given according to CCG-A9952 protocol. Results: Total/near-total resection in 105/227 (46.3%) without adjuvant treatment, while 49/227 patients (21.5%) underwent subtotal tumor resection followed by chemotherapy for big residual (n = 26). Follow-up only was indicated for asymptomatic/small residual (n = 23). The radiological diagnosis was set in 18/227 (7.9%) patients; 13/18 had optic pathway glioma. The 3-year overall survival (OS) was 87.3%- versus 65.5%-event free survival (EFS) for the whole study patients with a follow-up period of 1–5 years. The OS and EFS for patients who did surgery with no adjuvant treatment (n = 128) were, respectively, 95.2%-and 77.3%-versus 87.4%-and 65.1% for adjuvant chemotherapy group (n = 99); (P = 0.015 and P = 0.016 for OS and EFS, respectively). Conclusion: Pediatric LGGs comprise a wide spectrum of pathological and anatomical entities that carry a high rate of prolonged survival among children and adolescents. Surgical resection is the mainstay of treatment in most of tumors. Combined chemotherapy can be an acceptable alternative when surgery is not safely feasible.
Publication History
Article published online:
17 June 2021
© 2018. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Background: Pediatric gliomas comprise a clinically, histologically, and molecularly heterogeneous group of central nervous system tumors. The survival of children with gliomas influenced by histologic subtype, age, and extent of resection. Tumor grade emerged as the most determinant of survival except in the young age groups. The aim of this study was to evaluate the role of multidisciplinary therapeutic approach including surgery and chemotherapy, and their impact on the outcome in pediatric patients with low-grade glioma (LGG). Procedure: Study patients were prospectively enrolled onto the study. All patients were below 18-year-old, diagnosed as LGG between July 2007 and June 2012. Upfront surgical resection was attempted in all tumors other than optic pathway sites. Systemic chemotherapy was given according to CCG-A9952 protocol. Results: Total/near-total resection in 105/227 (46.3%) without adjuvant treatment, while 49/227 patients (21.5%) underwent subtotal tumor resection followed by chemotherapy for big residual (n = 26). Follow-up only was indicated for asymptomatic/small residual (n = 23). The radiological diagnosis was set in 18/227 (7.9%) patients; 13/18 had optic pathway glioma. The 3-year overall survival (OS) was 87.3%- versus 65.5%-event free survival (EFS) for the whole study patients with a follow-up period of 1–5 years. The OS and EFS for patients who did surgery with no adjuvant treatment (n = 128) were, respectively, 95.2%-and 77.3%-versus 87.4%-and 65.1% for adjuvant chemotherapy group (n = 99); (P = 0.015 and P = 0.016 for OS and EFS, respectively). Conclusion: Pediatric LGGs comprise a wide spectrum of pathological and anatomical entities that carry a high rate of prolonged survival among children and adolescents. Surgical resection is the mainstay of treatment in most of tumors. Combined chemotherapy can be an acceptable alternative when surgery is not safely feasible.
Introduction
Pediatric gliomas comprise group of central nervous system (CNS) tumors with clinical, histological, and molecular heterogeneous features. The survival of children with CNS gliomas is greatly affected by histological subtype, age, and extent of resection. Tumor grade is one of the most significant independent prognostic factors. Low-grade gliomas (LGGs) represent about 30% of gliomas and affect patients at a younger age than high-grade gliomas. They are commonly located in or close to the cerebral hemispheres.[1]
The 5-year overall survival (OS) and progression-free survival (PFS) rates range from 58%–72% to 37%–55%, respectively. Patients with LGGs may survive for up to 20 years, yet these tumors grow continuously.[2] [3] [4] They also tend to progress to a higher grade, leading to neurological disability, and ultimately to death. The optimal treatment of patients with LGG is still controversial.[5]
The usefulness of chemotherapy for patients who showed radiological progression after surgery and radiotherapy is well established, PCV (Procarbazine, CCNU, and Vincristine) and temozolomide (TMZ) yield similar response rates on doing follow-up imaging by computed tomography/magnetic resonance imaging (MRI) (45%–62%) and duration of response (10–24 months).[6] [7] [8] [9] [10] Protracted low doses of TMZ could offer potential advantages over standard doses.[11] Some studies found that low-grade tumors response is related to the genetic status; response rate after chemotherapy is higher in patients with t (1p-19q) than in those with the intact gene.[11]
Patients and Methods
The present study included LGG patients diagnosed and treated at the Children’s Cancer Hospital of Egypt (CCHE) during the period between 2007 and 2012. All patients were not previously treated and their age ≤18 years at diagnosis. According to the World Health Organization (WHO), Grade I-II supra- and infra-tentorial gliomas (pilocytic astrocytoma, fibrillary astrocytoma, pilomyxoid astrocytoma, oligodendroglioma, pleomorphic xanthoastrocytoma, subependymal giant cell astrocytoma, and optic pathway glioma [OPG]) were included. Patients with low-grade brain stem gliomas were not a candidate for the study. OS outcome defined as the time between the time of diagnosis and death, while event free survival (EFS) is the time between initial diagnosis and any event (tumor recurrence, progression, or death).
Treatment
Except for OPG, tumor tissue biopsy was taken whether stereotactic or open. Whenever safely feasible, complete surgical excision was attempted in every patient. Surgically ineligible patients were initiated on the CCG-A9952 protocol for LGG. Patients with small nonsymptomatic tumors were indicated for observation only. For radiologically diagnosed OPG chemotherapy was given if there was visual affection or subjected to regular time observation without any intervention if proved to have neurofibromatosis type 1 and vision was intact. Chemotherapy consisted of 10 weeks induction phase of vincristine and carboplatin with reevaluation done at its end and followed by eight cycles of maintenance chemotherapy. Follow-up was systematically conducted with MRI and fundus, visual field, visual acuity assessment in case of optic pathway glioma at regular checkpoints to evaluate tumor response and disease status. Salvage radiotherapy was indicated on disease progression while patients were under chemotherapy protocol (details of treatment are illustrated in [Figure 1]).
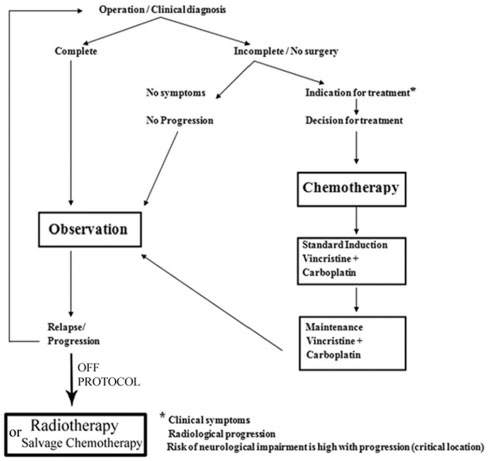
| Figure 1:Treatment algorithm in low-grade glioma patients
Statistical analysis
Age was used as a continuous variable (in the proportional hazards model). Estimates of survival probabilities (with 95% confidence intervals [95% CI]) were calculated using Kaplan–Meier product limit methodology and compared using a Wilcoxon log-rank test. Hazard rates were computed using a Cox proportional hazards model. Statistical significance defined as P ≤ 0.05. All analyses were completed using the SAS statistical software package. Alan Agresti; Xiao-Li Meng (November 2, 2012). Strength in Numbers: The Rising of Academic Statistics Departments in the US.[12]
Results
The study included 227 patients with slight male predominance (M/F: 1.2/1) and a median age of 6 years (range: 1–18 years), 34.7% were below 5 years, 61.3% from 5 to 14, and 4% of patients above 14-year-old at presentation.
Pilocytic astrocytoma was the most common pathological entity among cases (43.1%) followed by diffuse fibrillary astrocytoma (18.7%), OPG (5.8%), and ganglioglioma (5.3%); [Table 1].
|
Histological subtype |
Frequency, n (%) |
|---|---|
|
WHO – World Health Organization; LGG – Low grade glioma |
|
|
Pilocytic astrocytoma (WHO Grade I) |
97 (42.7) |
|
Diffuse fibrillary astrocytoma (WHO Grade II) |
42 (18.5) |
|
Pilomyxoid astrocytoma (WHO Grade II) |
37 (16.2) |
|
Ganglioglioma (WHO Grade I) |
18 (7.9) |
|
Optic pathway glioma |
13 (5.7) |
|
LGG (radiologically diagnosed) |
5 (2.2) |
|
LGG (pathologically unspecified) |
5 (2.2) |
|
Sub-ependymal giant cell astrocytoma |
|
|
(WHO Grade I) |
4 (1.7) |
|
Oligoastrocytoma (WHO Grade II) |
2 (0.8) |
|
Pleomorphic xanthoastrocytoma (WHO Grade II) |
2 (0.8) |
|
Desmoplastic infantile astrocytoma (WHO Grade I) |
1 (0.44) |
|
Choroid glioma (WHO Grade II) |
1 (0.44) |
|
Total |
227 (100) |
|
Tumor site |
Frequency, n (%) |
|---|---|
|
Cerebellar |
99 (43.6) |
|
Suprasellar |
31 (13.6) |
|
Optic pathway |
13 (5.7) |
|
Thalamic |
28 (12.3) |
|
Lobar |
43 (18.9) |
|
Cervico-spinal |
9 (3.96) |
|
Pineal body |
4 (1.76) |
|
Total |
227 (100) |
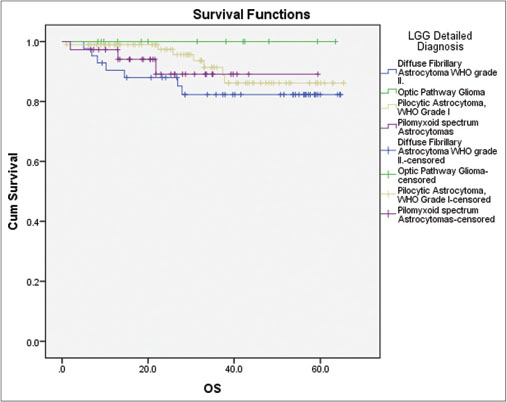
| Figure.2:Overall survival of study patients with different low-grade glioma subtypes
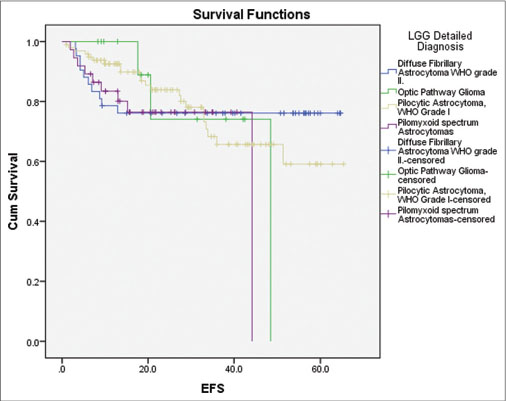
| Figure.3:Event-free survival of study patients with different low-grade glioma subtypes
According to tumor site, the best OS reported was associated with cerebellar tumors (93.4%) versus 73.3%-only for suprasellar sites, [Figure 4].
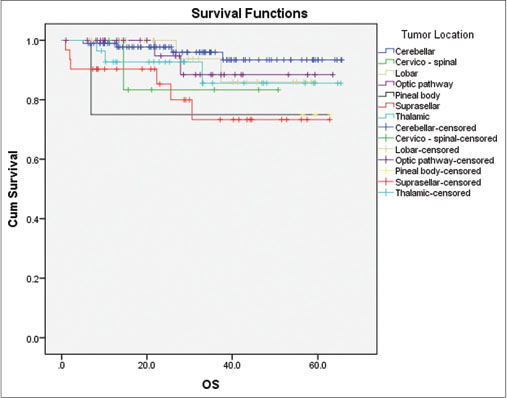
| Figure.4:Overall survival of study patients with different tumor site
Survival by site was further subclassified into two comparative groups excluding the spinal cord; group (1) included the cerebellum as well as cerebral tumors versus group (2) with tumors of limited resectability located in the deep midline structures as thalamus, hypothalamus, pineal body, suprasellar region, intraventricular, and in addition to the optic pathway. The 3-year OS was 96%-versus 86.8% (95% CI; 95.4–102.2 ± 1.67) in group (1) and group (2) respectively, with a statistically significant difference (P = 0.007). The difference in EFS was also significant between both groups; 80%-versus 66.9% (P = 0.05; 95%-CI: 75.3–86.2 ± 2.7), respectively [Figure 5] and [6].

| Figure.5:Comparative overall survival of two groups (1st group: Cerebellar and cerebral group and 2nd: Deep midline structure excluding spinal cord)

| Figure.6:Comparative Event-free survival of two groups (1st group: Cerebellar and cerebral group and 2nd: Deep midline structure excluding spinal cord
Discussion
The management of LGG is not unitary being one of the most controversial areas in clinical neuro-oncology and forming a composite of different challenges depending on the clinical presentation. LGGs can occur anywhere in the CNS and comprise multiple different tumor histologies making them difficult to categorize. Recent research has implicated activation of the RAS/RAF/MEK pathway in tumorigenesis of these tumors.[13]
The two most common LGG histologies in children are the pilocytic (WHO grade 1) and diffuse fibrillary astrocytoma (WHO Grade 2).
Cerebellar LGGs account for 15%–25% of all pediatric CNS tumors being the most prevalent location for LGG, followed by cerebral site (10%–15%), deep midline structures (10%–15%), OPGs (5%), and brain stem (2%–4%).[13] Same frequency order was also reported among our study patients as shown in [Table 2].
There will always be a dilemma in many patients about what is considered optimal management since there is no good evidence to support any single management to be adopted.[14]
Children with neurofibromatosis type 1 account for the majority (over 70%) of the optic pathway and hypothalamic gliomas.[15] Around 15%–20% of children with neurofibromatosis type 1 will develop an optic pathway/hypothalamic glioma. Fortunately, only about half of them will become symptomatic and require treatment, usually before the age of 5.[16] Low-grade brain stem gliomas include the dorsally exophytic, cervicomedullary, and focal brain stem gliomas and are to be distinguished from the more aggressive diffuse intrinsic brain stem gliomas.[13]
Pediatric LGGs are generally associated with long-term survival and low likelihood of related death in adulthood. Treatment strategies should, therefore, aim for disease control and emphasis on minimizing long-term toxicities.[17] Surveillance Epidemiology and End Results revealed a 20-year OS of 87% ± 0.8% and 12% ± 0.8%-cumulative incidence of death in pediatric LGG. Prognostic factors included the age of diagnosis, histology, WHO grade, primary tumor site, radiation, and degree of initial resection, and the year of diagnosis in univariate analysis.[17] In the study results, the 3-year OS was 87.3% for the whole patients group.
The treatment decision for children with subtotal resection has been controversial. If the likelihood of functional impairment is minimal and the neurosurgeon thinks it is feasible, a repeat surgery can be attempted to remove the residual tumor.[18] Others advocate a “wait and see approach” with follow-up brain MRI at 3–6-month intervals.[19]
Previous studies reported ≤90%-OS rates at 10 years from diagnosis for patients with completely resected tumors.[13] Our data also revealed that patients who underwent surgical resection without adjuvant treatment had OS of 95.2%-and 77.3%-EFS, versus 87.4%-and 65.1%-only for patients needed adjuvant chemotherapy (P = 0.015 and P = 0.016 for OS and EFS; respectively). Both literature data and our study results are in support of surgery as the mainstay of therapy till present.
On the other hand, most optic pathway, hypothalamic, deep midline, and brain stem gliomas with minimal resectability are difficult to treat and deserve special attention.[13] Our review of CCHE cases had the same conclusion as well. Survival outcome was much lower for deeply located and irresectable tumors in comparison to the relatively more superficial and accessible tumors (OS: 86.8% vs. 96%, respectively; P = 0.007). The difference was also significant for EFS between both groups (EFS: 66.9% vs. 80%, respectively; P = 0.05).
Currently, combination chemotherapy is recommended as front-line adjuvant treatment for progressive or recurrent LGG.
Recently, investigators concluded that chemotherapy was well tolerated in children with LGGs treated with Vinblastine once weekly for 70 weeks. Disease stabilization was achieved in 87.0% of study patients with a favorable toxicity profile and a maintained quality of life. Five-year OS and PFS rates were 94.4%- (95% CI, 88.5%–100%) and 53.2% (95% CI, 41.3%–68.5%), respectively. Patients with NF1 had a significantly better PFS (85.1%; 95% CI, 68.0%–100%) compared to patients without NF1 (42.0%; 95% CI, 29.1%–60.7%; P = 0.012). Age <3 href="https://www.thieme-connect.com/products/ejournals/html/10.4103/ijmpo.ijmpo_79_17#JR_20" xss=removed>20]
Radiotherapy used as second-line can also improve OS, yet it is associated with more frequent and significant long-term toxicities such as neurocognitive and endocrine disorders.[13] The administration of radiation was the greatest risk of death in multivariate analysis of OS (hazard ratio = 3.9).[17] Increased mortality in children treated with radiotherapy is likely to be a combination of both selection bias for children harder to have their disease controlled by other measures and radiation induced mortality (increased risk for second malignant neoplasia and vasculopathy).[17]
Considering the high survival outcome rates in LGGs of the pediatric and adolescent age groups, treatment strategies should, therefore, aim for disease control with an emphasis on minimizing long-term treatment induced toxicities.[17]
Conclusion
Pediatric LGGs comprise a wide spectrum of pathological and anatomical entities that carry a high rate of prolonged survival among children and adolescents. Surgical resection is the mainstay of treatment in most of tumors. Combined chemotherapy can be an acceptable alternative when surgery is not safely feasible and on recurrence.
Conflict of Interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank Mahmed Elbealtaegy, Mohamed Saaed Zaghalol, Amal Mosaeb.
References
- Duffau L, Capelle L. Preferential brain locations of low-grade gliomas. Cancer 2004; 100: 2622-6
- Claus EB, Black PM. Survival rates and patterns of care for patients diagnosed with supratentorial low-grade gliomas: Data from the SEER program, 1973-2001. Cancer 2006; 106: 1358-63
- Mandonnet E, Delattre JY, Tanguy ML, Swanson KR, Carpentier AF, Duffau H. et al. Continuous growth of mean tumor diameter in a subset of grade II gliomas. Ann Neurol 2003; 53: 524-8
- Rees J, Watt H, Jäger HR, Benton C, Tozer D, Tofts P. et al. Volumes and growth rates of untreated adult low-grade gliomas indicate risk of early malignant transformation. Eur J Radiol 2009; 72: 54-64
- Schiff D, Brown PD, Giannini C. Outcome in adult low-grade glioma: The impact of prognostic factors and treatment. Neurology 2007; 69: 1366-73
- Soffietti R, Rudà R, Bradac GB, Schiffer D. PCV chemotherapy for recurrent oligodendrogliomas and oligoastrocytomas. Neurosurgery 1998; 43: 1066-73
- van den Bent MJ, Kros JM, Heimans JJ, Pronk LC, van Groeningen CJ, Krouwer HG. et al. Response rate and prognostic factors of recurrent oligodendroglioma treated with procarbazine, CCNU, and vincristine chemotherapy. Dutch Neuro-oncology Group. Neurology 1998; 51: 1140-5
- van den Bent MJ, Taphoorn MJ, Brandes AA, Menten J, Stupp R, Frenay M. et al. Phase II study of first-line chemotherapy with temozolomide in recurrent oligodendroglial tumors: The European Organization for Research and Treatment of Cancer Brain Tumor Group Study 26971. J Clin Oncol 2003; 21: 2525-8
- Pace A, Vidiri A, Galiè E, Carosi M, Telera S, Cianciulli AM. et al. Temozolomide chemotherapy for progressive low-grade glioma: Clinical benefits and radiological response. Ann Oncol 2003; 14: 1722-6
- Quinn JA, Reardon DA, Friedman AH, Rich JN, Sampson JH, Provenzale JM. et al. Phase II trial of temozolomide in patients with progressive low-grade glioma. J Clin Oncol 2003; 21: 646-51
- Kaloshi G, Benouaich-Amiel A, Diakite F, Taillibert S, Lejeune J, Laigle-Donadey F. et al. Temozolomide for low-grade gliomas: Predictive impact of 1p/19q loss on response and outcome. Neurology 2007; 68: 1831-6
- Agrasti A, Meng X. Strengh in numbers:The rising of academic statistics department in U.S 2012. p.177.
- Sievert AJ, Fisher MJ. Pediatric low-grade gliomas. J Child Neurol 2009; 24: 1397-408
- Whittle IR. The dilemma of low grade glioma. J Neurol Neurosurg Psychiatry 2004; 75 (02) Suppl ii31-6
- Listernick R, Charrow J, Tomita T, Goldman S. Carboplatin therapy for optic pathway tumors in children with neurofibromatosis type-1. J Neurooncol 1999; 45: 185-90
- Czyzyk E, Józwiak S, Roszkowski M, Schwartz RA. Optic pathway gliomas in children with and without neurofibromatosis 1. J Child Neurol 2003; 18: 471-8
- Bandopadhayay P, Bergthold G, London WB, Goumnerova LC, Morales La Madrid A, Marcus KJ. et al. Long-term outcome of 4,040 children diagnosed with pediatric low-grade gliomas: An analysis of the Surveillance Epidemiology and End Results (SEER) database. Pediatr Blood Cancer 2014; 61: 1173-9
- Palma L, Celli P, Mariottini A. Long-term follow-up of childhood cerebellar astrocytomas after incomplete resection with particular reference to arrested growth or spontaneous tumour regression. Acta Neurochir (Wien) 2004; 146: 581-8
- Saunders DE, Phipps KP, Wade AM, Hayward RD. Surveillance imaging strategies following surgery and/or radiotherapy for childhood cerebellar low-grade astrocytoma. J Neurosurg 2005; 102 (02) Suppl 172-8
- Lassaletta A, Scheinemann K, Zelcer SM, Hukin J, Wilson BA, Jabado N. et al. Phase II weekly vinblastine for chemotherapy-naïve children with progressive low-grade glioma: A Canadian pediatric brain tumor consortium study. J Clin Oncol 2016; 34: 3537-43
Address for correspondence
Publication History
Article published online:
17 June 2021
© 2018. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2,
Noida-201301 UP, India
| Figure 1:Treatment algorithm in low-grade glioma patients
| Figure.2:Overall survival of study patients with different low-grade glioma subtypes
| Figure.3:Event-free survival of study patients with different low-grade glioma subtypes
| Figure.4:Overall survival of study patients with different tumor site
| Figure.5:Comparative overall survival of two groups (1st group: Cerebellar and cerebral group and 2nd: Deep midline structure excluding spinal cord)
| Figure.6:Comparative Event-free survival of two groups (1st group: Cerebellar and cerebral group and 2nd: Deep midline structure excluding spinal cord
References
- Duffau L, Capelle L. Preferential brain locations of low-grade gliomas. Cancer 2004; 100: 2622-6
- Claus EB, Black PM. Survival rates and patterns of care for patients diagnosed with supratentorial low-grade gliomas: Data from the SEER program, 1973-2001. Cancer 2006; 106: 1358-63
- Mandonnet E, Delattre JY, Tanguy ML, Swanson KR, Carpentier AF, Duffau H. et al. Continuous growth of mean tumor diameter in a subset of grade II gliomas. Ann Neurol 2003; 53: 524-8
- Rees J, Watt H, Jäger HR, Benton C, Tozer D, Tofts P. et al. Volumes and growth rates of untreated adult low-grade gliomas indicate risk of early malignant transformation. Eur J Radiol 2009; 72: 54-64
- Schiff D, Brown PD, Giannini C. Outcome in adult low-grade glioma: The impact of prognostic factors and treatment. Neurology 2007; 69: 1366-73
- Soffietti R, Rudà R, Bradac GB, Schiffer D. PCV chemotherapy for recurrent oligodendrogliomas and oligoastrocytomas. Neurosurgery 1998; 43: 1066-73
- van den Bent MJ, Kros JM, Heimans JJ, Pronk LC, van Groeningen CJ, Krouwer HG. et al. Response rate and prognostic factors of recurrent oligodendroglioma treated with procarbazine, CCNU, and vincristine chemotherapy. Dutch Neuro-oncology Group. Neurology 1998; 51: 1140-5
- van den Bent MJ, Taphoorn MJ, Brandes AA, Menten J, Stupp R, Frenay M. et al. Phase II study of first-line chemotherapy with temozolomide in recurrent oligodendroglial tumors: The European Organization for Research and Treatment of Cancer Brain Tumor Group Study 26971. J Clin Oncol 2003; 21: 2525-8
- Pace A, Vidiri A, Galiè E, Carosi M, Telera S, Cianciulli AM. et al. Temozolomide chemotherapy for progressive low-grade glioma: Clinical benefits and radiological response. Ann Oncol 2003; 14: 1722-6
- Quinn JA, Reardon DA, Friedman AH, Rich JN, Sampson JH, Provenzale JM. et al. Phase II trial of temozolomide in patients with progressive low-grade glioma. J Clin Oncol 2003; 21: 646-51
- Kaloshi G, Benouaich-Amiel A, Diakite F, Taillibert S, Lejeune J, Laigle-Donadey F. et al. Temozolomide for low-grade gliomas: Predictive impact of 1p/19q loss on response and outcome. Neurology 2007; 68: 1831-6
- Agrasti A, Meng X. Strengh in numbers:The rising of academic statistics department in U.S 2012. p.177.
- Sievert AJ, Fisher MJ. Pediatric low-grade gliomas. J Child Neurol 2009; 24: 1397-408
- Whittle IR. The dilemma of low grade glioma. J Neurol Neurosurg Psychiatry 2004; 75 (02) Suppl ii31-6
- Listernick R, Charrow J, Tomita T, Goldman S. Carboplatin therapy for optic pathway tumors in children with neurofibromatosis type-1. J Neurooncol 1999; 45: 185-90
- Czyzyk E, Józwiak S, Roszkowski M, Schwartz RA. Optic pathway gliomas in children with and without neurofibromatosis 1. J Child Neurol 2003; 18: 471-8
- Bandopadhayay P, Bergthold G, London WB, Goumnerova LC, Morales La Madrid A, Marcus KJ. et al. Long-term outcome of 4,040 children diagnosed with pediatric low-grade gliomas: An analysis of the Surveillance Epidemiology and End Results (SEER) database. Pediatr Blood Cancer 2014; 61: 1173-9
- Palma L, Celli P, Mariottini A. Long-term follow-up of childhood cerebellar astrocytomas after incomplete resection with particular reference to arrested growth or spontaneous tumour regression. Acta Neurochir (Wien) 2004; 146: 581-8
- Saunders DE, Phipps KP, Wade AM, Hayward RD. Surveillance imaging strategies following surgery and/or radiotherapy for childhood cerebellar low-grade astrocytoma. J Neurosurg 2005; 102 (02) Suppl 172-8
- Lassaletta A, Scheinemann K, Zelcer SM, Hukin J, Wilson BA, Jabado N. et al. Phase II weekly vinblastine for chemotherapy-naïve children with progressive low-grade glioma: A Canadian pediatric brain tumor consortium study. J Clin Oncol 2016; 34: 3537-43