 PDF
PDF  Views
Views  Share
Share


Malignant gastric teratoma in a 3-month-old infant
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2015; 36(04): 271
DOI: DOI: 10.4103/0971-5851.171554

Publication History
Article published online:
12 July 2021
© 2015. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
A 3-month-old boy presented with a rapidly growing abdominal mass noticed by his mother since 1-week, with no other significant history.
On examination, the child had a large, firm, nontender mass extending from the left hypochondrium to the right. Lymphadenopathy or ascites was absent. Alpha-fetoprotein (AFP) was markedly elevated at 18,055 ng/mL (normal 0.2-9.0 ng/mL) with normal beta human chorionic gonadotropin level.
Contrast enhanced tomography of the abdomen and chest revealed a large retroperitoneal heterogeneous mass pushing the left kidney inferiorly and displacing the gut to the right [Figure 1].

| Fig. 1 Axial contrast enhanced computed tomography of abdomen showing a large heterogeneous mass pushing the left kidney inferiorly and displacing the gut, no evidence of calcification
On exploration, a large intraperitoneal exophytic mass of size 8 cm × 9 cm × 8 cm was seen arising from the greater curvature and the posterior wall of the stomach occupying whole of the lesser sac [Figure 2]. It had variegated consistency with no involvement of adjacent structures and lymphadenopathy. The tumor was completely excised along with the involved gastric wall. Stomach was repaired in two layers.
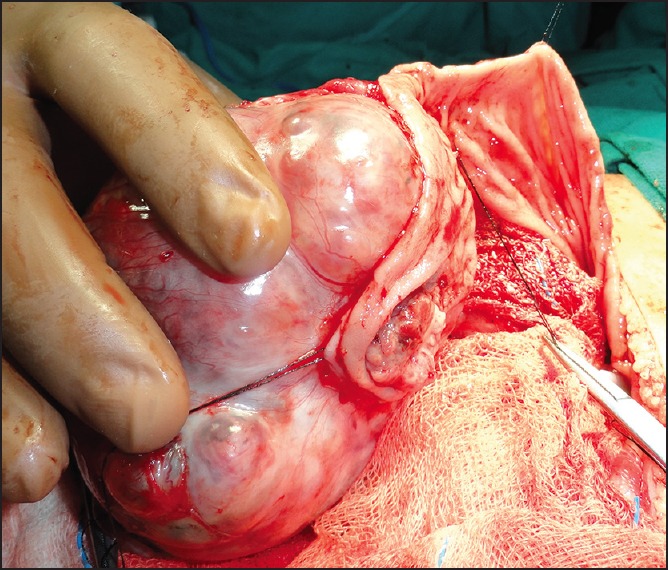
| Fig. 2 Intraoperative photograph demonstrating large mass arising from greater curvature and posterior wall of stomach
Histopathology revealed cystic, solid teratoid neoplasm, and a diagnosis of grade III immature teratoma was made. The tumor was seen invading the wall of the stomach and the resection margin of the stomach was free.
Postoperatively child remained healthy, and AFP levels came down to 5300 ng/mL. Child has been on regular follow-up for past 2 years with no recurrence.
| Fig. 1 Axial contrast enhanced computed tomography of abdomen showing a large heterogeneous mass pushing the left kidney inferiorly and displacing the gut, no evidence of calcification