 PDF
PDF  Views
Views  Share
Share


Isolated Oculomotor Palsy Due to Extramedullary Plasmacytoma in the Sphenoid Sinus
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2020; 41(02): 285-286
DOI: DOI: 10.4103/ijmpo.ijmpo_94_19
Sir,
Extramedullary plasmacytomas (EMPs) are localized tumors composed of monoclonal plasma cells in an extraskeletal area constituting 3% of all plasma cell neoplasms. A 75-year-old male presented with diplopia on horizontal gaze and headache for 1 month. His medical history was unremarkable. He was a smoker for 35 years (pack-year: 105). He had complete ptosis; dilated pupil (right 5 mm and left 3 mm); absent direct and indirect light reflexes, and limitation of adduction, depression, and elevation in the right eye. Fundus and rest of the systemic examination was normal. He had mild normocytic normochromic anemia, with high erythrocyte sedimentation rate. Biochemical parameters showed mild renal failure (serum creatinine – 1.6 mg%), reversed albumin/globulin ratio, and hypercalcemia. Magnetic resonance imaging of the brain showed a lesion in the sphenoid sinus measuring 4.2 cm × 3.4 cm × 3 cm extending into the sellar and suprasellar regions and clivus bone, which was heterogeneously hyperintense on T2 and isointense on T1 with contrast enhancement [Figure 1a] and [b]. The lesion was extending to the bilateral cavernous sinus encasing the cavernous portion of the right internal carotid artery for approximately 210° [Figure 1c] [d] [e]. Multiple focal lesions in the skull vault were seen. Skull X-ray showed multiple lytic lesions [Figure 1f]. A transnasal biopsy of the lesion showed plasmacytoma [Figure 1g] and [h]. Further investigations for multiple myeloma showed a monoclonal gammopathy on serum protein electrophoresis, Bence Jones protein in the urine, and 42% plasma cells in bone marrow study. A diagnosis of multiple myeloma stage with EMD was made, and the patient was started on chemotherapy with dexamethasone, cyclophosphamide, and bortezomib. When followed up after 6 months, the patient had no headache or diplopia and had radiological improvement (reduction in the size of the lesion). EMP generally displays a destructive course. EMP can be localized in one region or occur as a component of a systemic plasma cell dyscrasia. EMP associated with multiple myeloma has a bad prognosis when compared to solitary EMP. Sphenoid sinus is an extremely rare localization for an EMP.[1] Sphenoid sinus lesions have multiple benign and neoplastic causes.[2] Hence, it is important for clinicians to be aware of such unusual presentations of a common disease. This case highlights the need to consider EMP and coexisting multiple myeloma in patients with sphenoid sinus lesions.
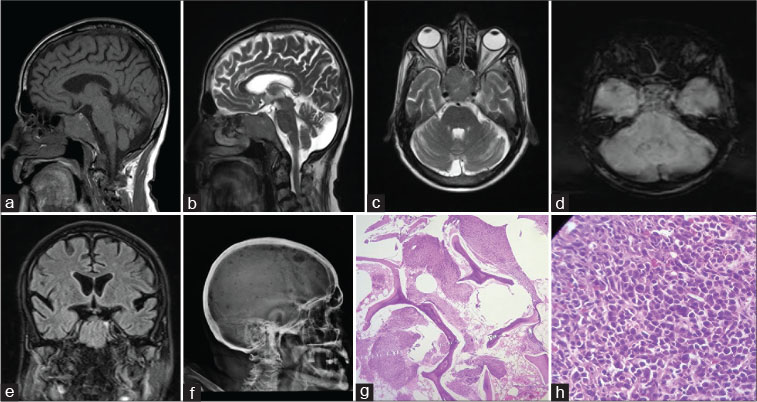
| Figure 1: Magnetic resonance imaging brain showing a lesion in the sphenoid sinus measuring 4.2 cm × 3.4 cm × 3 cm extending into the sellar and suprasellar regions and clivus bone, which was isointense on T1 (a) and hyperintense on T2 (b) with contrast enhancement. The lesion was extending to the bilateral cavernous sinus encasing the cavernous portion of the right internal carotid artery for 210° (c). Susceptibility images showing blooming (d). Coronal T2 image showing the lesion (e). Skull X-ray showing lytic lesions (f). Hematoxylin and eosin staining showing neoplastic plasma cells (g and h)
Publication History
Received: 08 April 2019
Accepted: 04 August 2019
Article published online:
23 May 2021
© 2020. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Sir,
Extramedullary plasmacytomas (EMPs) are localized tumors composed of monoclonal plasma cells in an extraskeletal area constituting 3% of all plasma cell neoplasms. A 75-year-old male presented with diplopia on horizontal gaze and headache for 1 month. His medical history was unremarkable. He was a smoker for 35 years (pack-year: 105). He had complete ptosis; dilated pupil (right 5 mm and left 3 mm); absent direct and indirect light reflexes, and limitation of adduction, depression, and elevation in the right eye. Fundus and rest of the systemic examination was normal. He had mild normocytic normochromic anemia, with high erythrocyte sedimentation rate. Biochemical parameters showed mild renal failure (serum creatinine – 1.6 mg%), reversed albumin/globulin ratio, and hypercalcemia. Magnetic resonance imaging of the brain showed a lesion in the sphenoid sinus measuring 4.2 cm × 3.4 cm × 3 cm extending into the sellar and suprasellar regions and clivus bone, which was heterogeneously hyperintense on T2 and isointense on T1 with contrast enhancement [Figure 1a] and [b]. The lesion was extending to the bilateral cavernous sinus encasing the cavernous portion of the right internal carotid artery for approximately 210° [Figure 1c] [d] [e]. Multiple focal lesions in the skull vault were seen. Skull X-ray showed multiple lytic lesions [Figure 1f]. A transnasal biopsy of the lesion showed plasmacytoma [Figure 1g] and [h]. Further investigations for multiple myeloma showed a monoclonal gammopathy on serum protein electrophoresis, Bence Jones protein in the urine, and 42% plasma cells in bone marrow study. A diagnosis of multiple myeloma stage with EMD was made, and the patient was started on chemotherapy with dexamethasone, cyclophosphamide, and bortezomib. When followed up after 6 months, the patient had no headache or diplopia and had radiological improvement (reduction in the size of the lesion). EMP generally displays a destructive course. EMP can be localized in one region or occur as a component of a systemic plasma cell dyscrasia. EMP associated with multiple myeloma has a bad prognosis when compared to solitary EMP. Sphenoid sinus is an extremely rare localization for an EMP.[1] Sphenoid sinus lesions have multiple benign and neoplastic causes.[2] Hence, it is important for clinicians to be aware of such unusual presentations of a common disease. This case highlights the need to consider EMP and coexisting multiple myeloma in patients with sphenoid sinus lesions.
| Figure 1: Magnetic resonance imaging brain showing a lesion in the sphenoid sinus measuring 4.2 cm × 3.4 cm × 3 cm extending into the sellar and suprasellar regions and clivus bone, which was isointense on T1 (a) and hyperintense on T2 (b) with contrast enhancement. The lesion was extending to the bilateral cavernous sinus encasing the cavernous portion of the right internal carotid artery for 210° (c). Susceptibility images showing blooming (d). Coronal T2 image showing the lesion (e). Skull X-ray showing lytic lesions (f). Hematoxylin and eosin staining showing neoplastic plasma cells (g and h)
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
References
- Ozdemir S, Tarkan O, Tuncer U, Sürmelioğlu O, Doğrusöz M, Ergin M. A case of extramedullary plasmacytoma in the sphenoid sinus with unilateral loss of vision. J Craniomaxillofac Surg 2013; 41: 140-3
- Marcolini TR, Safraider MC, Socher JA, Lucena GO. Differential diagnosis and treatment of isolated pathologies of the sphenoid sinus: Retrospective study of 46 cases. Int Arch Otorhinolaryngol 2015; 19: 124-9
Address for correspondence
Publication History
Received: 08 April 2019
Accepted: 04 August 2019
Article published online:
23 May 2021
© 2020. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
| Figure 1: Magnetic resonance imaging brain showing a lesion in the sphenoid sinus measuring 4.2 cm × 3.4 cm × 3 cm extending into the sellar and suprasellar regions and clivus bone, which was isointense on T1 (a) and hyperintense on T2 (b) with contrast enhancement. The lesion was extending to the bilateral cavernous sinus encasing the cavernous portion of the right internal carotid artery for 210° (c). Susceptibility images showing blooming (d). Coronal T2 image showing the lesion (e). Skull X-ray showing lytic lesions (f). Hematoxylin and eosin staining showing neoplastic plasma cells (g and h)
References
- Ozdemir S, Tarkan O, Tuncer U, Sürmelioğlu O, Doğrusöz M, Ergin M. A case of extramedullary plasmacytoma in the sphenoid sinus with unilateral loss of vision. J Craniomaxillofac Surg 2013; 41: 140-3
- Marcolini TR, Safraider MC, Socher JA, Lucena GO. Differential diagnosis and treatment of isolated pathologies of the sphenoid sinus: Retrospective study of 46 cases. Int Arch Otorhinolaryngol 2015; 19: 124-9