 PDF
PDF  Views
Views  Share
Share


Innovative use of the fiberoptic bronchoscope
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2012; 33(04): 233-235
DOI: DOI: 10.4103/0971-5851.107090 CASE REPORT
Abstract
Tracheostomy can be challenging, especially in the presence of edema or infiltrative malignancy. We present a case in which a fiberoptic bronchoscope that is routinely used for difficult intubation helped to locate the trachea in an emergency situation. A 50 year-old male, a diagnosed case of anaplastic carcinoma of thyroid, presented with respiratory distress and was immediately taken to the operating theater for an emergency tracheostomy. Following an inhalational induction, the patient was intubated with an endotracheal tube. Surgical tracheostomy was extremely difficult as, on neck exploration, there was a plaque of disease infiltrating various tissue planes. When even after considerable dissection the trachea could not be located, we passed a fiberoptic bronchoscope through the endotracheal tube. This helped as it was seen as a trans- illumination and the tracheal position could be confirmed. The rest of the tracheostomy was uneventful.
Publication History
Article published online:
20 July 2021
© 2012. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Tracheostomy can be challenging, especially in the presence of edema or infiltrative malignancy. We present a case in which a fiberoptic bronchoscope that is routinely used for difficult intubation helped to locate the trachea in an emergency situation. A 50 year-old male, a diagnosed case of anaplastic carcinoma of thyroid, presented with respiratory distress and was immediately taken to the operating theater for an emergency tracheostomy. Following an inhalational induction, the patient was intubated with an endotracheal tube. Surgical tracheostomy was extremely difficult as, on neck exploration, there was a plaque of disease infiltrating various tissue planes. When even after considerable dissection the trachea could not be located, we passed a fiberoptic bronchoscope through the endotracheal tube. This helped as it was seen as a trans- illumination and the tracheal position could be confirmed. The rest of the tracheostomy was uneventful.
INTRODUCTION
Surgical tracheostomy, which is a commonly performed lifesaving procedure, has a low complication rate. However, sometimes, it may become difficult as in the case of morbid obesity, any neck swelling causing displacement of the trachea or tumor invading the trachea where locating the trachea can be difficult. In such situations, fiberoptic bronchoscope may be helpful in correctly identifying the trachea thus avoiding a potential complication. The aim of this case report is to describe an effective and safe use of fiberoptic bronchoscope, aiding a difficult tracheostomy.
CASE REPORT
A 50-year old male, a diagnosed case of anaplastic carcinoma of thyroid, presented with a large thyroid swelling causing respiratory distress. A decision for emergency tracheostomy was made by the surgical team and the patient was transferred to the operation theater. Comorbidities included hypertension, for which he was on regular medications. Chest X-ray showed tracheal deviation to the right [Figure 1] and Hopkins (indirect laryngoscopy) examination showed decreased right vocal cord movement. All other investigations were normal.

| Fig. 1 Chest X-ray showing tracheal deviation
The procedure was explained to the patient and informed consent was taken. All standard monitors were attached and basal vital parameters were noted. Intravenous access was secured and a difficult intubation trolley was kept ready in the theater with all airway adjuvants.
Induction
After preoxygenation, inhalational induction was performed with sevoflurane and direct laryngoscopy was performed. The vocal cords were sprayed with 4% lignocaine and the airway was secured with an endotracheal tube. Anesthesia was maintained with a mixture of oxygen and air with sevoflurane and intravenous drugs including fentanyl and vecuronium, which were given after confirmation of endotracheal tube in the trachea by auscultation and waveform capnography.
Surgical difficulty
On neck exploration, there was a plaque of disease infiltrating various tissue planes. The trachea that appeared to be shifted on the right side could not be seen or felt because of disease plaque. The endotracheal tube that was passed also could not be felt. Usual test of tracheal puncture, with aspiration of air through syringe, was also not helpful. Therefore, it was considered unsafe to make an incision blindly on a structure that was assumed to be the trachea.
To locate the trachea, a fiberoptic bronchoscope was then introduced through the endotracheal tube, which helped, as it was seen as a trans-illumination, and the tracheal position could be confirmed [Figure 2]. The rest of the tracheostomy was uneventful. Endotracheal tube was then withdrawn over the fiberoptic bronchoscope and a tracheostomy tube was introduced into the trachea. The placement of the tracheostomy tube was confirmed with waveform capnography and then the fiberoptic bronchoscope was removed.
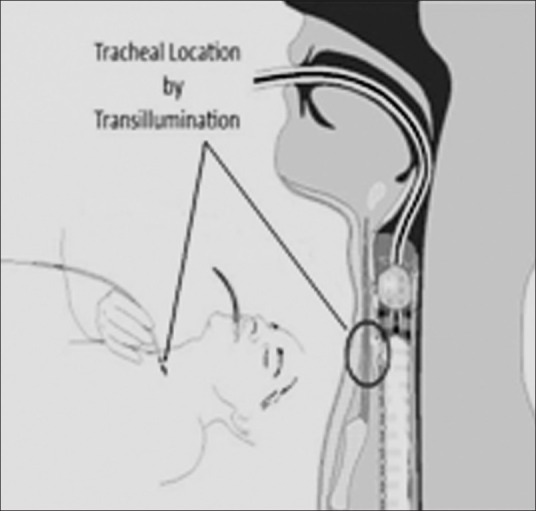
| Fig. 2 Tracheal location by trans-illumination
Postprocedure, the neuromuscular blockade was reversed and the patient was shifted to the intensive care unit for further management.
DISCUSSION
Our case is that of a patient suffering from anaplastic carcinoma of the thyroid where we used the fiberoptic bronchoscope to aid an emergency difficult tracheostomy.
Anaplastic thyroid CA (ATC) is the most aggressive and lethal form of thyroid cancer. Fortunately, it accounts for only 1–2% of all thyroid tumors.[1] Most patients with ATC demonstrate local compressive symptoms such as dysphagia, dysphonia, stridor and neck pain due to direct invasion of the surrounding tissue such as fat, trachea, esophagus and larynx.[2,3] Death is usually due to extensive local disease causing airway obstruction. Airway obstruction can occur by three mechanisms: external compression of trachea, intraluminal tumor extension or bilateral vocal cord paralysis. Management of ATC is mostly palliative, which includes preventing death from asphyxiation and securing a safe airway. Airway management can be elective or emergent, depending on patient's presentation. Patients with stridor or rapidly growing tumor are candidates for tracheostomy, which may be challenging, and airway should first be secured in these cases under direct vision or with the use of a fiberoptic bronchoscope[4] Awake emergency tracheostomy in such patients could be tricky and can lead to life-threatening complications.
Our patient who was a known case of ATC presented with stridor and needed an emergency tracheostomy. Securing the airway was uneventful, but even in experienced hands it was difficult to locate the trachea. The fiberoptic bronchoscope that was introduced through the endotracheal tube helped in locating the trachea and to overcome the problem.
Open tracheostomy is a commonly performed procedure with a complication rate of 6–66%.[5] This rate may increase in difficult cases like morbid obesity, cervical stiffness, tumor invading trachea or displacement of trachea. Fiberoptic bronchoscope forms very important equipment for difficult intubation and has been routinely used while performing percutaneous tracheostomy. Light wand-guided percutaneous tracheostomy has previously been shown to decrease complication rate and has also been useful in difficult open tracheostomy cases.[6,7]
We used the principle of trans-illumination to locate the trachea with a fiberoptic bronchoscope, which proved to be very useful during a difficult tracheostomy. Therefore, in such cases where open tracheostomy can be challenging, we should be aware of this technique that is simple yet helpful in locating the trachea and may prove to be a good aid.
This case is presented to share one of the novel applications of the fiberoptic bronchoscope in case of difficult tracheostomy.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
| Fig. 1 Chest X-ray showing tracheal deviation
| Fig. 2 Tracheal location by trans-illumination