 PDF
PDF  Views
Views  Share
Share


Immature teratoma at umbilicus region presenting as exomphalos: A case report with review of literature
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2014; 35(03): 231-233
DOI: DOI: 10.4103/0971-5851.142042
Abstract
Umbilical cord neoplasms are rare. Teratomas, which are accepted as the only true neoplasms at this site, are exceptional. These tumors are polymorphic in their presentation and are often associated with other abnormalities, with exomphalos being the most common abnormality. Histologically these tumors show mature tissues from all the three-germ layers. Immature elements as seen in our case are rare. Germ cells which have gone astray during embryonic development are thought to be the cells of origin of these tumors.
Publication History
Article published online:
19 July 2021
© 2014. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Umbilical cord neoplasms are rare. Teratomas, which are accepted as the only true neoplasms at this site, are exceptional. These tumors are polymorphic in their presentation and are often associated with other abnormalities, with exomphalos being the most common abnormality. Histologically these tumors show mature tissues from all the three-germ layers. Immature elements as seen in our case are rare. Germ cells which have gone astray during embryonic development are thought to be the cells of origin of these tumors.
INTRODUCTION
Teratomas are tumors composed of tissues from all the three-germ layers, often occurring in the gonads. Their occurrence in extragonadal sites is rare with umbilical cord being one such rare site. Review of literature showed only 16 cases of umbilical cord teratomas to have been reported so far, with five of them being associated with an exomphalos.[1,2,3,4,5,6] Herein we report a case of an immature teratoma of the umbilical cord in a preterm infant, which was misdiagnosed as an exomphalos on ultrasound, suggesting that an ultrasonographic in utero diagnosis of an abdominal wall mass with solid and cystic areas in the fetus should be viewed with suspicion.
CASE REPORT
A 22-year-old primigravida from rural setup went to an obstetrician in private practice for antenatal check-up. Ultrasound examination done as part of the check-up revealed a single live fetus of 20 weeks gestation with a small hypoechoic shadow in the anterior abdominal wall. No definite opinion was possible as the patient refused to undergo further investigations. She came for her next visit in the 9th month of gestation. Ultrasonography done then revealed a live fetus with an 112 mm × 80 mm × 58 mm mass protruding from the anterior abdominal wall with both hypoechoic and hyperechoic areas. A radiological diagnosis of an exomphalos was made. The obstetrician induced labor by administering misofestrone followed by misoprostol. The woman delivered a female baby weighing 2.650 kg with a mass protruding from the anterior abdominal wall along with a segment of small bowel.
The neonate was sent to a tertiary care hospital for specialist care on the 2nd day, wherein she developed bilious vomiting. Suspecting intestinal obstruction, emergency surgery was done. The surgeon found a partly skin covered nodular mass protruding from the anterior abdominal wall with the umbilical cord lateral to it, along with a normal segment of small bowel protruding out. Prominent veins were seen coursing over the anterior abdominal wall above the mass [Figure 1]. Intraoperatively the mass was found to contain nodules of adipose tissue covered over by skin with a peau de orange appearance along with firm gritty areas. It could be shelled out easily with attachment only at the umbilical ring. Duodenal atresia beyond the level of opening of the bile duct was noted intra-abdominally. A duodeno-duodenal anastamoses was done and the resected mass was sent for histopathological examination with a diagnosis of a teratoma. The neonate expired on the 2nd postoperative day due to hypothermia and sepsis.

| Figure 1:Clinical photograph at presentation ×1000
PATHOLOGIC FINDINGS
The specimen consisted of 10 cm × 7 cm × 5 cm gray-white to yellowish nodular soft tissue mass with a part of the umbilical cord attached to it. Some of the nodules were covered with skin. Cut section of the skin covered nodules revealed adipose tissue while the other nodules showed cystic spaces along with solid, firm to gritty areas. Cut section of the cord revealed three-blood vessels.
Histologically the mass showed skin with dermal appendages, respiratory and intestinal type of epithelia along with pancreatic tissue. Loose connective tissue, adipose tissue, bone, cartilage, glial tissue and choroid plexus were also seen with neuroepithelial tubules predominating [Figure 2].
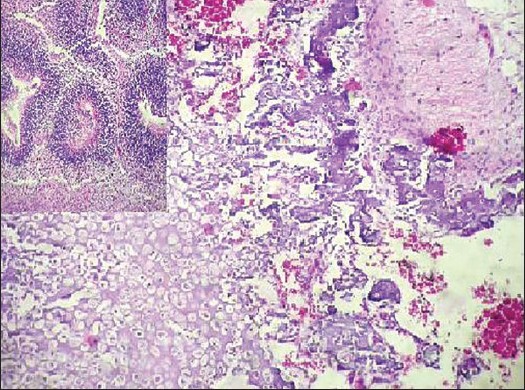
| Figure 2:Sections showing bone, cartilage and mature glial tissue. Inset showing neuroepithelial tubules (H and E, ×400)
Based on these features a diagnosis of an immature teratoma Grade II was made.
DISCUSSION
Teratomas are the only true neoplasms of the umbilical cord. Like all other extragonadal teratoma, they are thought to develop from pluri or toti potent cells with diploid chromosome set that have not yet undergone the first meiotic division, and show various cytogenetic abnormalities often involving Ch. 1 and 12 along with hypoploid and hypertriploid chromosome numbers.[7,8,9] They rarely contain immature elements as seen in our case.
Review of literature revealed 16 cases of umbilical cord teratomas identified at varying ages of gestation, ranging from 17 weeks to term. These tumors were polymorphic in presentation, with sizes ranging from 1.8 cm diameter to that of an infant's head and occurred along the entire length of the cord.[6]
Most of the cases (12/16) were in females, and most were recognized after term delivery.[1,2,3,5,6] Associated abnormalities were seen in 8/16 cases reported. Exomphalos was the most common abnormality (5/8 cases), followed by an umbilical hernia, exstrophy of the bladder and myelomeningocoel with hydrocephalous in others.[1,2,3,4,5,6] One of the cases with exomphalos was associated with trisomy 13.[5]
Derivatives from all the three-germ layers are present with mature tissues occurring in most of the cases. Immature elements as seen in our case have been described in three other cases.[1,2,7] Two of these cases were identified at 17 weeks of gestation and in these cases their occurrence could probably correspond to the developmental stage of the fetus.[6] Hartz and van der Sar reported the presence of immature elements in a term infant.[10] The child described by them had two lesions, one in the umbilical cord which was resected after birth and another in the liver which grew and disseminated, leading to death of the child at the age of 4 months.
Immature teratomas occurring in infants often contain embryonic appearing neuroglial or neuroepithelial components, which may coexist with mature tissues. Their presence, irrespective of the grade, is said to have no bearing on prognosis.[8]
With respect to the occurrence of two lesions in the case described by Hartz and van der Sar, the authors suggest that they could be independent tumors or that the tumor might have originated initially in the umbilical vein, part of which separated and got incorporated in the liver during the embryonal development.[10] Satgé et al. proposed that these two lesions may be due to the occurrence of two independent tumors or due to a metastatic teratoma originating from either of the sites, suggesting that not all teratomas of the umbilical cord are benign.[6]
Outcome in extragonadal teratomas is determined by the extent of resection of the tumor and presence of foci of yolk sac tumor in the neoplasm.[8] Presence of associated anomalies and surgical complications after correction of the congenital malformations also affect the outcome in these cases.
CONCLUSION
Umbilical cord teratomas are rare neoplasms which can be detected antenatally as solid and cystic masses simulating an exomphalos when present near the anterior abdominal wall, suggesting that a high index of suspicion is essential when an abdominal wall mass is detected in the fetus in utero. Prognosis in these cases is largely determined by the associated abnormalities.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Bilge CD, Naile BT, Esra SG, Zeynep Y, Ulviye Y. Prenataldiagnosis of fetal umbilical cord teratoma. Perinat Med 2014;3.
- Keene DJ, Shawkat E, Gillham J, Craigie RJ. Rare combination of exomphalos with umbilical cord teratoma. Ultrasound Obstet Gynecol 2012;40:481.
- Crahes M, Patrier S, Ickowicz V, Blondiaux E, Elbaz F, Diguet A, et al. Giant teratoma of the umbilical cord associated with foetal malformations: A morphological and cytogenetic study. Ann Pathol 2013;33:57-61.
- Del Sordo R, Fratini D, Cavaliere A. Teratoma of umbilical cord: A case report and literature review. Pathologica 2006;98:224-8.
- Hargitai B, Csabai L, Bán Z, Hetényi I, Szucs I, Varga S, et al. Rare case of exomphalos complicated with umbilical cord teratoma in a fetus with trisomy 13. Fetal Diagn Ther 2005;20:528-33.
- Satgé DC, Laumond MA, Desfarges F, Chenard MP. An umbilical cord teratoma in a 17-week-old fetus. Prenat Diagn 2001;21:284-8.
- Wagner H, Baretton GB, Schneiderbanger K, Nerlich A, Bise K, Löhrs U. Sex chromosome determination in extragonadal teratomas by interphase cytogenetics: Clues to histogenesis. Pediatr Pathol Lab Med 1997;17:401-12.
- Isaacs H Jr. Germ cell tumors. In: Gilbert-Barness E, editor. Potter′s Pathology of the Fetus, Infant and Child. 2 nd ed. China: Mosby Elsevier; 2007. p. 1690-707.
- Kreczy A, Alge A, Menardi G, Gassner I, Gschwendtner A, Mikuz G. Teratoma of the umbilical cord. Case report with review of the literature. Arch Pathol Lab Med 1994;118:934-7.
- ;Hartz PH, van der Sar A. Teratoma of the liver in an infant. Am J Clin Pathol 1945;15:1959-63.
| Figure 1:Clinical photograph at presentation ×1000
| Figure 2:Sections showing bone, cartilage and mature glial tissue. Inset showing neuroepithelial tubules (H and E, ×400)
References
- Bilge CD, Naile BT, Esra SG, Zeynep Y, Ulviye Y. Prenataldiagnosis of fetal umbilical cord teratoma. Perinat Med 2014;3.
- Keene DJ, Shawkat E, Gillham J, Craigie RJ. Rare combination of exomphalos with umbilical cord teratoma. Ultrasound Obstet Gynecol 2012;40:481.
- Crahes M, Patrier S, Ickowicz V, Blondiaux E, Elbaz F, Diguet A, et al. Giant teratoma of the umbilical cord associated with foetal malformations: A morphological and cytogenetic study. Ann Pathol 2013;33:57-61.
- Del Sordo R, Fratini D, Cavaliere A. Teratoma of umbilical cord: A case report and literature review. Pathologica 2006;98:224-8.
- Hargitai B, Csabai L, Bán Z, Hetényi I, Szucs I, Varga S, et al. Rare case of exomphalos complicated with umbilical cord teratoma in a fetus with trisomy 13. Fetal Diagn Ther 2005;20:528-33.
- Satgé DC, Laumond MA, Desfarges F, Chenard MP. An umbilical cord teratoma in a 17-week-old fetus. Prenat Diagn 2001;21:284-8.
- Wagner H, Baretton GB, Schneiderbanger K, Nerlich A, Bise K, Löhrs U. Sex chromosome determination in extragonadal teratomas by interphase cytogenetics: Clues to histogenesis. Pediatr Pathol Lab Med 1997;17:401-12.
- Isaacs H Jr. Germ cell tumors. In: Gilbert-Barness E, editor. Potter′s Pathology of the Fetus, Infant and Child. 2 nd ed. China: Mosby Elsevier; 2007. p. 1690-707.
- Kreczy A, Alge A, Menardi G, Gassner I, Gschwendtner A, Mikuz G. Teratoma of the umbilical cord. Case report with review of the literature. Arch Pathol Lab Med 1994;118:934-7.
- ;Hartz PH, van der Sar A. Teratoma of the liver in an infant. Am J Clin Pathol 1945;15:1959-63.