 PDF
PDF  Views
Views  Share
Share


Head and neck squamous cell carcinoma in chronic areca nut chewing Indian women: Case series and review of literature
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2012; 33(01): 32-35
DOI: DOI: 10.4103/0971-5851.96966
Abstract
Background: Head and neck squamous cell carcinoma (HNSCC) is an important public health problem in India. Several risk factors such as tobacco, human papilloma virus, alcohol, areca nut usage have been extensively studied as causative agents. Though Areca nut chewing is known cause of oral cancer, its association with hypopharynx cancer has not been previously reported. Since areca nut is mostly consumed along with tobacco, it is uncommon to find patients who consume the areca nut alone. Materials and Methods: This is a prospective case series of ten women who presented to us with HNSCC with history of chewing of areca nut alone for several years. We have excluded all those cases where areca nut was consumed along with tobacco in any form. The data were prospectively collected with regard to clinical parameters, duration and frequency of areca nut usage, the socio-economic status and education level. Results: All ten females had varying degree of submucous fibrosis and coexisting squamous cell carcinoma either in the oral cavity or hypopharynx. Submucous fibrosis was characterized by burning mouth, unhealthy oral mucosa, buried third molars, trismus, poor oral hygiene, etc. The disease presented in an advanced stage in majority of the cases. All patients were unaware of areca nut′s deleterious effects. Conclusion: Areca nut chewing is an important risk factor for HNSCC in females. Despite plethora of information, little importance is given to areca nut control in cancer prevention campaigns in India.
Publication History
Article published online:
13 April 2022
© 2012. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Background:
Head and neck squamous cell carcinoma (HNSCC) is an important public health problem in India. Several risk factors such as tobacco, human papilloma virus, alcohol, areca nut usage have been extensively studied as causative agents. Though Areca nut chewing is known cause of oral cancer, its association with hypopharynx cancer has not been previously reported. Since areca nut is mostly consumed along with tobacco, it is uncommon to find patients who consume the areca nut alone.
Materials and Methods:
This is a prospective case series of ten women who presented to us with HNSCC with history of chewing of areca nut alone for several years. We have excluded all those cases where areca nut was consumed along with tobacco in any form. The data were prospectively collected with regard to clinical parameters, duration and frequency of areca nut usage, the socio-economic status and education level.
Results:
All ten females had varying degree of submucous fibrosis and coexisting squamous cell carcinoma either in the oral cavity or hypopharynx. Submucous fibrosis was characterized by burning mouth, unhealthy oral mucosa, buried third molars, trismus, poor oral hygiene, etc. The disease presented in an advanced stage in majority of the cases. All patients were unaware of areca nut's deleterious effects.
Conclusion:
Areca nut chewing is an important risk factor for HNSCC in females. Despite plethora of information, little importance is given to areca nut control in cancer prevention campaigns in India.
INTRODUCTION
Several risk factors such as tobacco, human papilloma virus, areca nut, alcohol have been described in the literature as causative agents for head and neck squamous cell carcinoma (HNSCC). In recent years, areca nut consumption has been linked to oral cancer in studies from south east Asian countries.[1–5] Betel nut has a long history of use in south east Asian natives and is part of their culture and religion. Areca nut chewing is associated with acute as well as chronic effects. The acute effects are worsening of asthma, low blood pressure, and rapid heart beats[5,6] whereas chronic effects are oral submucous fibrosis (OSF), precancerous oral lesions, and squamous cell carcinoma. We report a series of female patients with head and neck cancer who had the habit of chewing only areca nut without any history of tobacco usage in any form. We present their clinical parameters, socioeconomic status, education level, duration, and frequency of areca nut chewing along with review of the literature. We also intend to highlight the association of hypopharynx carcinoma with areca nut chewing habit, which has not been studied in the literature so far.
MATERIALS AND METHODS
These are prospectively collected data of ten patients who presented to us with biopsy proven HNSCC and a history of areca nut chewing without any history of tobacco usage. We collected information on clinical parameters, duration, and frequency of areca nut chewing, socioeconomic status, and education level of the patients. Socioeconomic status was assessed using the updated Kuppuswamy socioeconomic status scale.[7]
RESULTS
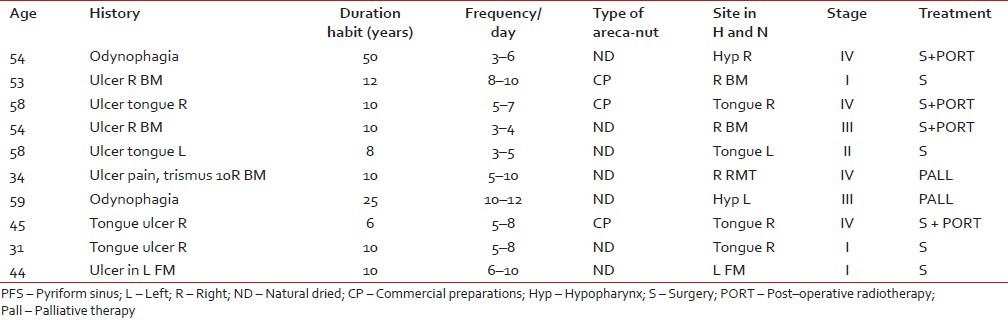
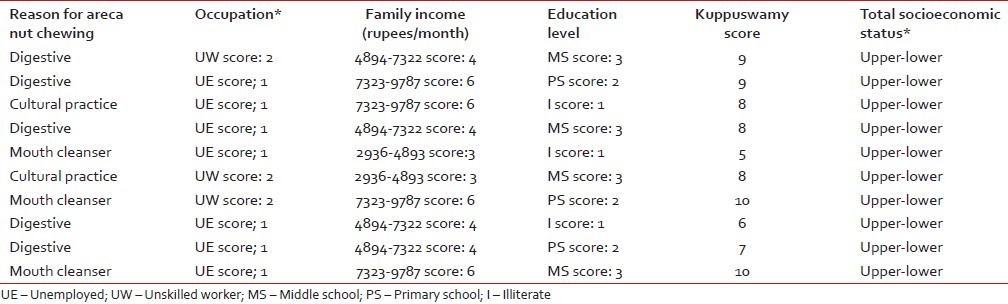
There were ten female patients [Table 1] with the mean age of 49 (ranging from 31 to 59 years). Two patients presented with hypopharynx cancer and eight had the lesions in oral cavity (four tongue, three buccal mucosa, and one floor of mouth). Amongst those with oral cancer, the most common complaint was that of a nonhealing ulcer in the oral cavity along with features of submucus fibrosis (trismus, white, and sensitive mucosa). OSF was present in all these cases, involving bilateral buccal mucosa, palate, and tongue. All patients complained of progressive inability to open mouth and sensitive mucosa (to hot and spicy foods) of varying degree [Figures [Figures11 and and2].2]. The mean duration of areca nuts chewing was 15.1 years (ranging from 6 to 50 years). Areca nut chewing habit had a wide variation in these cases, in terms of duration, frequency, socioeconomic status, and employment status. Most of the patients had the habit of areca nut chewing with an average of three to six times a day. The commonest form of areca nut chewed was the Natural Dried form (7/10 cases) and the rest three cases admitted to chew commercially prepared areca nut products [Table 1]. The patients belonged to the upper–lower socioeconomic category [Table 2] and were housewives. Amongst the eight oral cancer cases, tongue (4) was most frequently involved subsite followed by buccal mucosa (3) and floor of mouth (1). The oral hygiene in these patients was compromized due to trismus and painful ulcers. Tongue followed by buccal mucosa were the primary sites of oral carcinoma in chewers of commercially available areca nut products whereas hypopharynx was primary site in chewers of natural dried areca nut, in addition to buccal mucosa and tongue. There were lot of soft deposits, plaque, and calculus and the typical stain due to tobacco and betel quid (brownish black or yellowish brown) was not seen in these cases. Also, the typical incrustations on the soft tissue especially seen in Gutka chewers and chewers of pan with tobacco were absent on clinical examination in these cases. This suggested their “only areca nut” chewing habit. There was gross generalized attrition of teeth with exposed roots, wear facets, and root stumps, contributing to poor oral hygiene. There were two cases of SCC involving pyriform sinus (subsite of hypopharyx) that presented with odynophagia with an average duration of 45 days. One of the patients underwent total laryngectomy followed by radiation therapy, and one patient required only palliative care. The submucous fibrosis was seen to involve the entire upper aerodigestive tract in these cases. Intraoperative finding in patient undergoing total laryngectomy and laryngoscopic examination in the other patient showed extensive submucous fibrosis in the hypopharyngeal and laryngeal mucosa. In majority of the cases (6/10), the lesions were in an advanced stage requiring extensive surgical resection and reconstructions followed by aggressive adjuvant therapies. In two patients curative treatment was not possible and palliative chemotherapy was advised.
Table 1
Age, clinical details, site and treatment details of patients with head and neck cancer

| Fig. 1 Clinical presentation with variable degree of restricted mouth opening and ulcerative lesion

| Fig. 2 Clinical presentation with ulcerations, stains on teeth with attrition and poor oral hygiene
Table 2
Reason for areca nut chewing and socioeconomic status as per the Kuppuswamy scale
DISCUSSION
In contrast to the western literature wherein smoking, alcohol and human papilloma virus have been described as major risk factors for head and neck SCC,[8] smokeless tobacco, and areca nut chewing are predominant risk factors in India. Areca nut chewing is a unique problem in India and other Southeast Asian countries.[3,4] Areca nut is a highly addictive substance with the score for mean severity of dependence as 7.3 (in a range of 1–12) similar to the problematic use of amphetamines.[9] There have been reports of usage of these products in Asian migrants to the United States, the United Kingdom, Singapore, Australia, Germany, South Africa etc.[10–19] This habit is an important public health problem in Taiwan. Although, chewing areca nut has been found to be associated with oral cancer and recently with development of primary hepatocellular and esophageal carcinoma,[20,21] this was the first time we encountered a series of carcinoma of hypopharynx in areca nut chewers. Unlike tobacco, areca nut is portrayed as a safe mouth freshener; therefore, it is freely available and widely consumed. There are reports of areca nut addiction amongst children of south east Asian countries which results in oral cancer in the younger age. A study in Pakistan reported that school children at primary school level are areca nut addicts and 74% children used areca nut, 35% of them chewed betel quid daily.[22] The cases described in our study were middle-aged housewives with the chronic betel nut chewing habit. Due to the small sample size, dose–response assessment could not be made. The reasons for areca nut consumption in these cases were its psycho-stimulating effects causing a euphoric feeling, sweetening breath, as a digestive or as a cultural practice. The patients had a lower level of education and not aware of the deleterious effects associated with areca nut chewing habit. Psychopharmacological effects of areca nut have been described as a popular pleasure giving substance in South Asia and include increase in concentration, mild mood elevation, enhanced satisfaction after eating and relaxation.[4,23] It has varied psychological effects of which most predominant is the stimulating effect. Habituation and addiction to daily chewing of the quid has also been reported amongst the people hailing from the Gujarat state in India.[24,25] Majority of cases in our study were of tongue and buccal mucosa, in accordance with a study from South Africa.[5] The cause of submucous fibrosis is the excessive synthesis of collagen in the submucous tissues. In vitro studies with cultured fibroblasts have shown that areca nut alkaloids such as arecoline and its hydrolyzed product arecaidine stimulate proliferation and collagen synthesis in a dose-dependent manner, higher concentrations being cytotoxic.[26,27] Flavonoids, catechins, and tannins in areca nuts cause collagen fibers to crosslink, making them less susceptible to collagenase.[28] Furthermore, the extracts of areca nut and its components have been shown to be crucial in the pathogenesis of OSF and oral cancer by differentially inducing the dysregulation of cell cycle control mitochondrial membrane potential, depletion of cellular glutathione, and intracellular H2O2 production.[28] It has been estimated that people with OSF are 19.1 times more likely to develop oral cancer than those without it, after adjusting for other risk factors and another study describe a 7.6% rate of malignant transformation of OSF to frank carcinoma over a 10-year period.[29,30] We did not come across any other published report where areca nut has been linked to the hypopharynx cancer. The finding of the features of submucous fibrosis in the hypopharynx and larynx mucosa is a sparsely reported feature in chronic areca nut chewers. Similarly, association of hypopharynx cancer with submucous fibrosis of oral cavity is an uncommon problem that poses challenge during evaluation and treatment of these cancers. Pyriform sinuses are the sites of maximal salivary contact because of mechanical reasons. This can explain association of pyriform sinus cancer in those chewing areca nut.
CONCLUSION
Areca nut chewing is an important risk factor in the genesis of oral potentially malignant and malignant lesions in Indian women. Although there is a need to establish the carcinogenic effects of areca nut at a genetic or molecular level in these cases, wide spread health education programs are necessary to reach both urban- and rural-based populations in education and motivation against the habit of chewing areca nuts. Its deleterious effect needs to be highlighted in all cancer prevention campaign. The sale and production of areca nut should be discouraged.
Footnotes
Source of Support: Nil
REFERENCES
| Fig. 1 Clinical presentation with variable degree of restricted mouth opening and ulcerative lesion
| Fig. 2 Clinical presentation with ulcerations, stains on teeth with attrition and poor oral hygiene