 PDF
PDF  Views
Views  Share
Share


Four rare extranodal sites seen on FDG PET/CT in a single patient of disseminated lymphoma
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2013; 34(02): 101-103
DOI: DOI: 10.4103/0971-5851.116189
Abstract
Extranodal disease refers to lymphomatous infiltration of anatomic sites other than lymph nodes. With the advent of FDG PET/CT for staging, rare sites of extranodal disease have been documented. We report a case of Non- Hodgkin′s lymphoma with four rare extranodal sites, namely adrenal, peripheral nerves, pancreas and prostate, in the same patient, detected on FDG PET/CT imaging.
Publication History
Article published online:
20 July 2021
© 2013. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Extranodal disease refers to lymphomatous infiltration of anatomic sites other than lymph nodes. With the advent of FDG PET/CT for staging, rare sites of extranodal disease have been documented. We report a case of Non- Hodgkin's lymphoma with four rare extranodal sites, namely adrenal, peripheral nerves, pancreas and prostate, in the same patient, detected on FDG PET/CT imaging.
INTRODUCTION
FDG PET/CT is commonly used for staging and treatment response assessment in lymphomas, as in helps in picking up primary sites, nodes and extranodal sites in a single study. This also leads to uncovering of rare sites of lymphomatous involvement. Our case similarly shows four rare extranodal sites in a case of Non Hodgkin's lymphoma on PET/CT.
CASE REPORT
A 25-year-old gentleman, on anti-retroviral treatment for immunopositivity for HIV, since two years, presented to our institution 4 months back, with history of unexplained fever, weight loss and bilateral axillary swellings. On examination he had palpable bilateral axillary nodes. Recent CD4 count was 550 cells/mm3. A biopsy from the left axillary node confirmed it to be Non-Hodgkin's lymphoma (NHL) B cell type. Patient was then referred for a baseline whole body 18-F Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography (FDG PET/CT) study. Maximum intensity projection (MIP) images [Figure 1a] revealed multiple foci of increased tracer uptake in bilateral cervical, axillary, mediastinal and retroperitoneal regions. In addition, there were foci of intense uptake on the left side of abdomen (arrow) and in the pelvis (arrow head), which appeared to be due to physiological tracer excretion into the urinary bladder. Axial fused PET/CT images revealed multiple enlarged FDG avid bilateral axillary and mediastinal nodes. In addition, FDG uptake was seen in enlarged bilateral adrenal glands, left being more than right [Figure 1b, arrows]. There was focal FDG uptake seen in the body of pancreas on axial-fused PET/CT images [Figure 1c, arrow]. FDG uptake in the retroperitoneal region corresponded on CT and fused PET/CT images to exiting nerve roots from lumbar vertebrae [Figure [Figure2a2a and andb,b, arrow]. Also, the FDG uptake in the pelvis which appeared to be excreted tracer in bladder, was in fact seen in the enlarged prostate gland on CT and fused PET/CT images [Figure [Figure2c2c and andd,d, arrow]. Patient received two cycles of intravenous bolus chemotherapy regimen, R-EPOCH (Rituximab with etoposide, vincristine, doxorubicin, cyclophosphamide, and prednisone) with methotrexate, after which he was referred for a FDG PET/CT study for treatment response assessment. Post-treatment FDG PET/CT study revealed no abnormal focus of FDG uptake in the entire body, suggestive of complete metabolic and morphological response to treatment [Figure 3, MIP image].
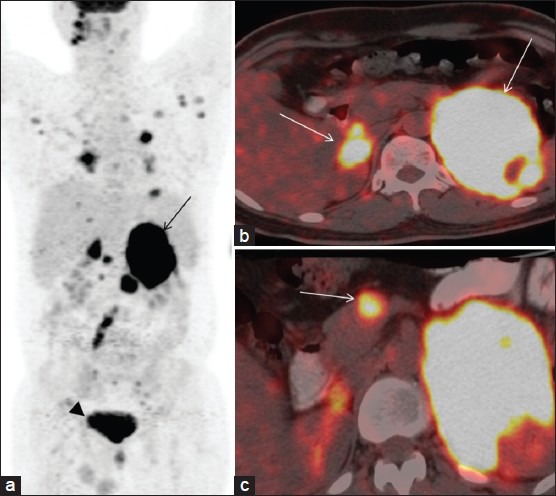
| Fig. 1 (a) MIP image showing abnormal tracer foci in abdomen (arrow) and pelvis (arrowhead) (b) Axial fused image showing intense tracer uptake in bilateral adrenal glands (arrows) (c) Axial fused image showing tracer uptake in body of pancreas (arrow)
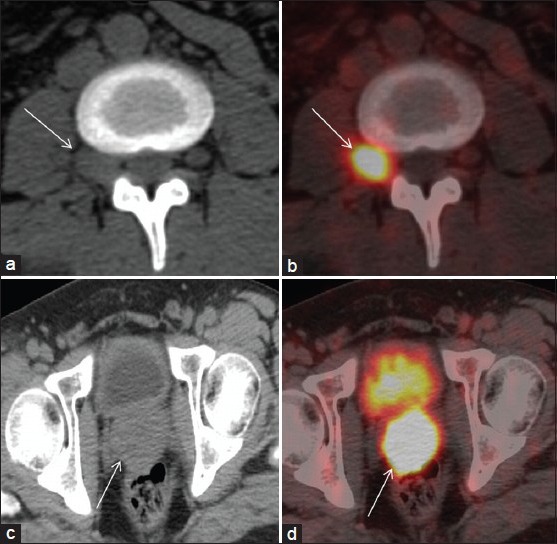
| Fig. 2 (a) Axial CT image showing enlarged exiting nerve root with loss of surrounding fat planes (arrow) (b) Axial fused image showing intense uptake in exiting nerve root (arrow) (c) Axial CT image showing enlarged prostate gland (arrow) (d) Axial fused image showing uptake in the prostate gland (arrow)

| Fig. 3 Post-treatment MIP image showing no abnormal tracer uptake
DISCUSSION
Rare sites of extranodal involvement like skin, stomach, small intestine, kidney, bone, ovary, adrenal, peripheral nerves and prostate have been documented in the existing literature[1] Non-Hodgkin's lymphoma can involve adrenal in almost 25% of cases, either with nodal involvement or as primary adrenal lymphoma.[2] Neurolymphomatosis (NL) is an uncommon syndrome of cranial or peripheral nerve root dysfunction secondary to infiltration by B cell Non-Hodgkin's lymphoma and is an extremely rare manifestation of lymphoma.[3] Although CT and MRI have been used for detection and guiding biopsy in NL, recent reports have demonstrated the value of FDG PET/CT in NL.[4,5] There has been only one case report showing involvement of lumbar plexus on FDG PET/CT,[6] with this being the second one. Similarly, prostatic involvement is rarely encountered, with primary prostatic lymphomas representing approximately 0.2-0.8% of extranodal lymphomas, with urinary tract obstruction being the commonest presentation.[7] Secondary pancreatic involvement has been reported in only 0.2-2% of patients with NHL, out of which only two cases had B cell lymphoma, ours being the third case.[8] All the reports in literature give one rare site of extranodal involvement or a rare site of primary origin of lymphoma. There are no studies which document four rare extranodal sites in the same patient. Uncovering such rare sites in one single patient once again highlights the role of FDG PET/CT in staging of lymphomas. Lymphomas, both Hodgkins and Non-Hodgkins type, can have varied presentations and hence a whole body metabolic imaging with CT fusion is essential to pick up all the sites of lymphomatous involvement to design appropriate treatment regimens. Also, it serves as a baseline, which can be compared to the post-treatment study for assessing response, as in this case, wherein a post-treatment PET/CT study shows complete metabolic response to treatment.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
| Fig. 1 (a) MIP image showing abnormal tracer foci in abdomen (arrow) and pelvis (arrowhead) (b) Axial fused image showing intense tracer uptake in bilateral adrenal glands (arrows) (c) Axial fused image showing tracer uptake in body of pancreas (arrow)
| Fig. 2 (a) Axial CT image showing enlarged exiting nerve root with loss of surrounding fat planes (arrow) (b) Axial fused image showing intense uptake in exiting nerve root (arrow) (c) Axial CT image showing enlarged prostate gland (arrow) (d) Axial fused image showing uptake in the prostate gland (arrow)
| Fig. 3 Post-treatment MIP image showing no abnormal tracer uptake