 PDF
PDF  Views
Views  Share
Share


Extra-axial cerebello pontine angle medulloblastoma: A rare site of tumor
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2011; 32(02): 123-124
DOI: DOI: 10.4103/0971-5851.89801
Publication History
Article published online:
06 August 2021
© 2011. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Sir,
Medulloblastoma is a common tumor of the posterior fossa, representing 20–25% of all pediatric neoplasms.[1]
The tumor often occurs in the cerebellar vermis and at the apex of the fourth ventricle.[1,2] There are only a few reported cases of cerebellopontine (CP)-angle medulloblastoma in the literature, with most being intra-axial. The extra-axial site of this tumor remains a rarity.[1,3]
This 4-year-old girl presented with left hemicranial headache followed by facial asymmetry with deviation of angle of mouth for 1 month. There was no other significant history.
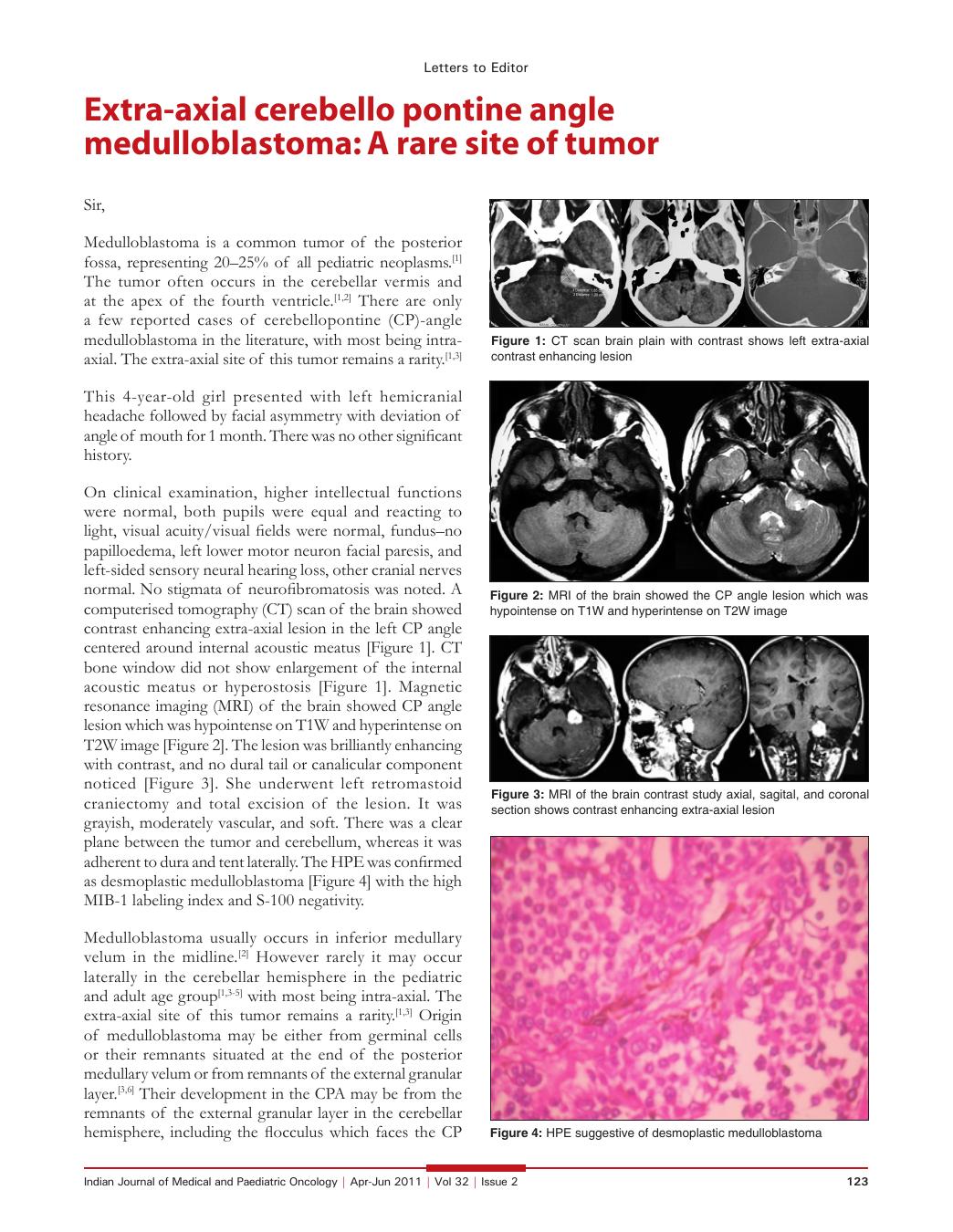
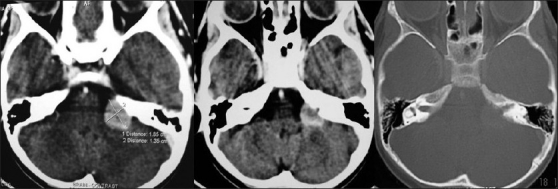
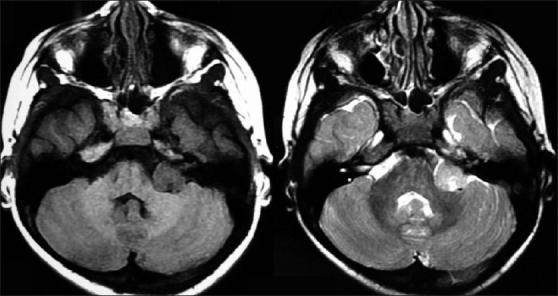
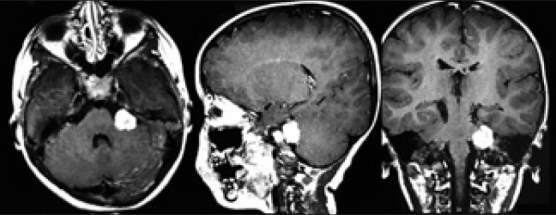
On clinical examination, higher intellectual functions were normal, both pupils were equal and reacting to light, visual acuity/visual fields were normal, fundus-no papilloedema, left lower motor neuron facial paresis, and left-sided sensory neural hearing loss, other cranial nerves normal. No stigmata of neurofibromatosis was noted. A computerised tomography (CT) scan of the brain showed contrast enhancing extra-axial lesion in the left CP angle centered around internal acoustic meatus [Figure 1]. CT bone window did not show enlargement of the internal acoustic meatus or hyperostosis [Figure 1]. Magnetic resonance imaging (MRI) of the brain showed CP angle lesion which was hypointense on T1W and hyperintense on T2W image [Figure 2]. The lesion was brilliantly enhancing with contrast, and no dural tail or canalicular component noticed [Figure 3]. She underwent left retromastoid craniectomy and total excision of the lesion. It was grayish, moderately vascular, and soft. There was a clear plane between the tumor and cerebellum, whereas it was adherent to dura and tent laterally. The HPE was confirmed as desmoplastic medulloblastoma [Figure 4] with the high MIB-1 labeling index and S-100 negativity.
| Fig. 1 CT scan brain plain with contrast shows left extra-axial contrast enhancing lesion
| Fig. 2 MRI of the brain showed the CP angle lesion which was hypointense on T1W and hyperintense on T2W image
| Fig. 3 MRI of the brain contrast study axial, sagital, and coronal section shows contrast enhancing extra-axial lesion
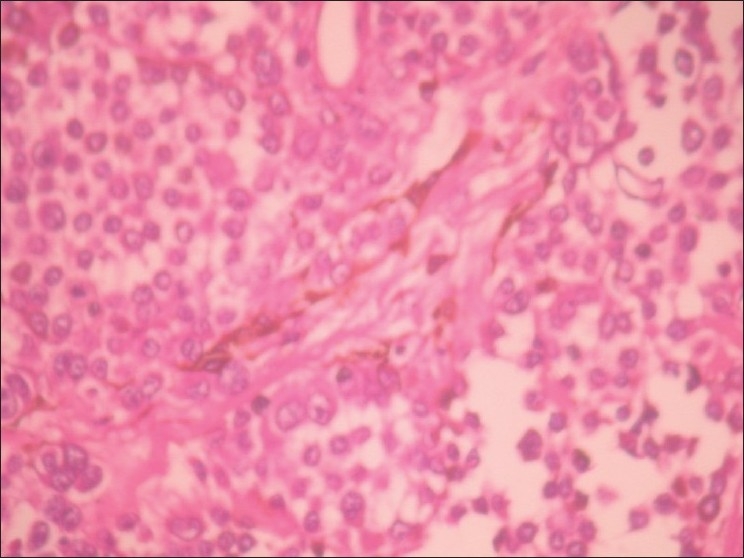
| Fig. 4 HPE suggestive of desmoplastic medulloblastoma
Medulloblastoma usually occurs in inferior medullary velum in the midline.[2] However rarely it may occur laterally in the cerebellar hemisphere in the pediatric and adult age group[1,3–5] with most being intra-axial. The extra-axial site of this tumor remains a rarity.[1,3] Origin of medulloblastoma may be either from germinal cells or their remnants situated at the end of the posterior medullary velum or from remnants of the external granular layer.[3,6] Their development in the CPA may be from the remnants of the external granular layer in the cerebellar hemisphere, including the flocculus which faces the CP angle.[3,6] In the CP angle, medulloblastomas though fifth, sixth, and eighth cranial nerves are frequently involved, these nerves were spared in this patient.[5,7] CP angle medulloblastomas are very rare with nearly 36 cases published in the literature[1,3,5] of which only 10 are in adults.[1,3,5,7] The lack of association with any cerebellar tissue and the extra-axial location of the tumor made our patient's case quite rare. However, they are likely under-reported owing to publication bias and must be considered in the differential diagnosis of extra-axial CP angle lesions.
REFERENCES
| Fig. 1 CT scan brain plain with contrast shows left extra-axial contrast enhancing lesion
| Fig. 2 MRI of the brain showed the CP angle lesion which was hypointense on T1W and hyperintense on T2W image
| Fig. 3 MRI of the brain contrast study axial, sagital, and coronal section shows contrast enhancing extra-axial lesion
| Fig. 4 HPE suggestive of desmoplastic medulloblastoma