 PDF
PDF  Views
Views  Share
Share


Changing trends of chronic myeloid leukemia in greater Mumbai, India over a period of 30 years
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2011; 32(02): 96-100
DOI: DOI: 10.4103/0971-5851.89792
Abstract
Background: Little is known about burden of chronic myeloid leukemia (CML) in India. There is a recent interest to observe incidence and mortality because of advent of new diagnostic and treatment policies for CML. Materials and Methods: We extracted data from the oldest population-based cancer registry of Mumbai for 30 years period from 1976−2005 to observe incidence and mortality rates of CML. We classified the data into four age groups 0−14, 15−29, 30−54 and 55−74 to observe incidence rates in the respective age groups. Results: The age specific rates were highest for the age group of 55−74 years. No significant change in trends of CML was observed for 30 years period. However, there was a significant reduction in incidence rate for recent 15-years period (Estimated average annual percentage change=-3.9). No significant reduction in mortality rate was observed till 2005. Conclusion: The study demonstrates that age-specific rates for CML are highest in age group of 55-74 years, although they are lower compared to western populations. Significant reduction in incidence of CML in recent periods might be because of reduced misclassification of leukemias. The data of CML has to be observed for another decade to witness reduction in mortality because of changes in treatment management.
Publication History
Article published online:
06 August 2021
© 2011. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Background:
Little is known about burden of chronic myeloid leukemia (CML) in India. There is a recent interest to observe incidence and mortality because of advent of new diagnostic and treatment policies for CML.
Materials and Methods:
We extracted data from the oldest population-based cancer registry of Mumbai for 30 years period from 1976−2005 to observe incidence and mortality rates of CML. We classified the data into four age groups 0–14, 15–29, 30–54 and 55–74 to observe incidence rates in the respective age groups.
Results:
The age specific rates were highest for the age group of 55–74 years. No significant change in trends of CML was observed for 30 years period. However, there was a significant reduction in incidence rate for recent 15-years period (Estimated average annual percentage change=-3.9). No significant reduction in mortality rate was observed till 2005.
Conclusion:
The study demonstrates that age-specific rates for CML are highest in age group of 55-74 years, although they are lower compared to western populations. Significant reduction in incidence of CML in recent periods might be because of reduced misclassification of leukemias. The data of CML has to be observed for another decade to witness reduction in mortality because of changes in treatment management.
INTRODUCTION
Chronic myeloid leukemia (CML) is a relatively rare disease with a worldwide annual incidence rate ranging from less than 1.0 to 2.0 per 100,000 persons. CML represents 14% of all cases of leukemia (Leukemia and Lymphoma Society, 2004). About 3% of childhood leukemias are CML, and 10% of cases of CML occur in children aged 5–20 years.[1] Highest rates were reported for Switzerland, USA, Italy, Australia, Germany, and UK. Lower rates were reported for Netherlands, Sweden, China, and India.[2–4] It is slightly more common in males than in females. In general, the male predominance has been estimated to be 1.3-1.4 to 1.[5] Most of the CML cases arise from an acquired genetic abnormality, which is a result of translocation between chromosome 22 and chromosome 9, in a bone marrow stem cell, known as the Philadelphia chromosome.[1] This translocation results when the Abelson (ABL) gene from chromosome 9 merges with the breakpoint cluster region (BCR) gene on chromosome 22, resulting in a BCR-ABL fusion gene on 22q11 that encodes for uncontrolled tyrosine kinase activity (Leukemia and Lymphoma Society, 2005).
The other important risk factors for CML are high doses of ionizing radiation and occupational exposure to benzene. This is evident from 20–25 fold increase in the incidence of all the leukemias among atomic bomb survivors.[6,7] Limited studies are reported to discuss other risk factors for CML. Alcohol,[8] obesity, and adulthood weight gain[9] are reported to play important roles in CML risk.
Diagnostic testing plays a key role in the management of CML. Diagnosis of CML has been rapidly changing over the years with sensitive diagnostic tests. Earlier, diagnosis only included complete blood count (CBC), comprising differential and platelet count, marrow aspiration, and marrow biopsy. Recent development in diagnosis for CML involves more sensitive tests such as standard cytogenetics, fluorescent in-situ hybridization (FISH) and quantitative polymerase chain reaction (PCR).[6]
Traditionally, CML was treated with interferon and chemotherapy drugs such as hydroxyurea. The real key breakthroughs in the treatment of this disease came about in the late 1980's and early 1990's with bone marrow transplants,[10,11] followed by the introduction of imatinib in the late 1990′s, which has dramatically impacted the survival of patients. Recent studies have reported 10 year survival to be around 80%.[12–15] Such marked improvements in the management of CML have resulted in increasing the survival, and hence, decline in mortality has been reported in certain population mainly from the developed countries.[5] Recently in developing countries, particularly in India, there has been improvement in diagnosis with genetic testing available in some centers from 2001. Similarly, treatment management has also shown improvement with success of imatinib as first line therapy. This might have resulted in reducing misclassification of leukemias and changes in the incidence and mortality of CML. However, there have been few reports on the epidemiology of CML to reflect these changes.
To study the descriptive epidemiology of CML from 1976 to 2005 in Mumbai, we used data of the Mumbai population-based cancer registry, the first cancer registry established in India. We focused our analysis to compare and contrast temporal differences in CML incidence among different age groups.
MATERIALS AND METHODS
We obtained the incidence and mortality cases of CML from Mumbai population-based cancer registry records. The Mumbai Cancer registry collects data from different sources on all cancer sites in defined geographical regions of Mumbai.[16] We extracted CML incident cases from Mumbai Population based Cancer Registry database having International Classification of Diseases - 9 (ICD - 9) code 204.1 and to the ages 0-74 years to examine incidence rates over a 30-year time period. We also analyzed mortality rates for the more recent 15-year period (1991-2005). The corresponding population at risk was obtained from census data.[17]
The crude incidence rates were obtained by dividing the incident cases in a defined time period to the population at risk in the same time period. The age-specific rate and age-adjusted rate were estimated as per the method described in cancer incidence in five continents.[18] The average annual percentage change over 30 years and for most recent 15 years (1991-2005) was obtained by fitting a log-linear model to age and time.[19]
To compare the incidence rates of CML observed in Mumbai with developed countries, we extracted data of CML from Surveillence, Epidemiology, and End Results (SEER) database for the year 2003-2007. The age-adjusted rates truncated for age groups 0-14, 15-29, 30-54, and 55-74 using world standard population were computed to compare the rates in these age groups and were labeled as pediatric, young, adult, and geriatric population, respectively.
RESULTS
The total number of incident CML cases in males over the period of 30 years(1976-2005) was 6.1% of 4264 total leukemia cases [Table 1], whereas the total leukemia cases in females was 2594 of which 6.7% were CML cases [Table 2]. The age-specific incidence rates of CML shows increase in the rates with age for both males and females.
Table 1
Incident CML cases and age specific incidence rates per 100,000 for pediatric, young, adult and geriatric population stratified by six calendar years from 1976-2005 in Mumbai, India
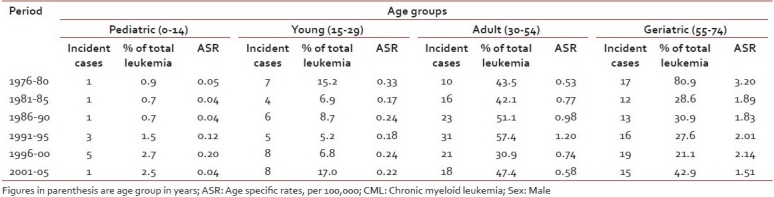
Table 2
Incident CML cases and age specific incidence rates per 100,000 for pediatric, young, adult and geriatric population stratified by six calendar years from 1976-2005 in Mumbai, India
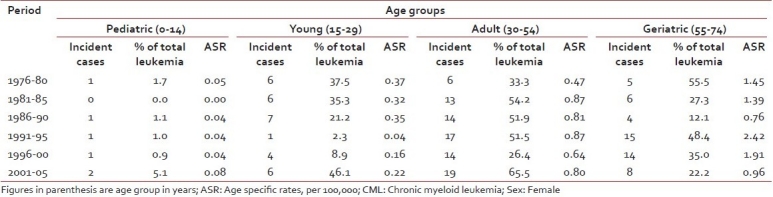
The incidence rate of CML has decreased in recent period (1991–2005) in Mumbai (age 0-74) for both males (EAPC=-2.9; 95% CI=-4.6 to -1.0) and females (EAPC=-2.5; 95% CI=-7.5 to -0.2). Similarly, decrease in incidence rate was observed for overall 30-year period; however, the decrease was not statistically significant [Table 3].
Table 3
EAPC of CML for 30 year period (1976-2005) and for more recent periods (1991-2005) by gender, in Mumbai India
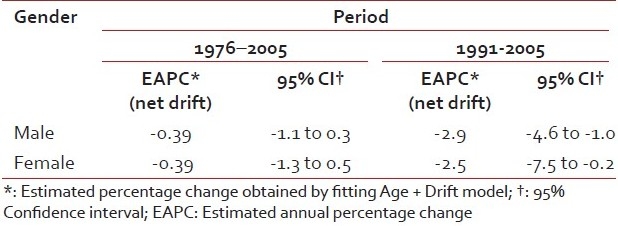
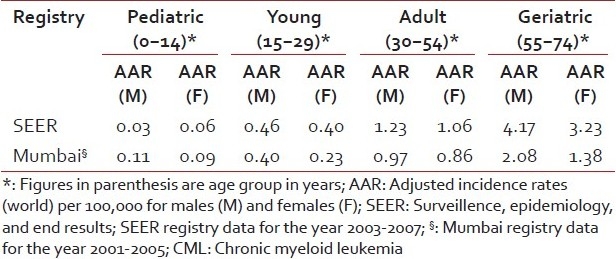
Table 4 shows the age-adjusted mortality rate for males and females for recent period (1991–2005). The mortality rate for males ranged from 0.48 to 0.45 per 100,000 and that of females was 0.41 to 0.31 per 100,000 for 15-year period. The age-adjusted incidence rate (AAR) of CML was higher in pediatric group, almost comparable in young and adult population, whereas it was lower in geriatric population (Incidence rate ratio=0.42) in Mumbai compared to that observed by SEER registries [Table 5].
Table 4
Age adjusted (world) mortality rates per 100,000 by gender for CML in Mumbai for recent period (1991-2005)
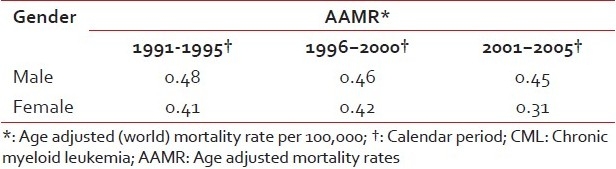
Table 5
Comparison of age adjusted (world) incidence rates truncated to age groups 0-14, 15-29, 30-54 and 55-74 (AAR), stratified by gender in Mumbai and SEER Registries for Pediatric, young, adult and geriatric populations
DISCUSSION
The results of the present study are derived from population-based cancer registry, which has registered cancer cases since 1965. There has been no change in the registry catchment area during the study period, with a relatively small percentage of cases (approximately 3%) - registered on the basis of a death certification only. Data of Mumbai population-based cancer registry has shown to be reasonably reliable and complete.[20] The registry data have met the stringent criteria for inclusion in successive Volumes of Cancer Incidence in Five Continents published by International Agency for Research in Cancer (IARC)[18,21]
To study burden and trend of CML in developing countries, we have utilized the demonstrable quality data of Mumbai Cancer Registry. The incidence of CML in developing countries is low (AAR=0.71 in males and 0.53 per 100,000 in females) compared to US (AAR=2.0 in males and 1.1 per 100,000 in females) and many other developed countries.[4,5,16] In contrast to observation from large series of hospital data which suggests that the peak age for occurrence of CML is in younger age group, our population based data suggests that ASR of CML are highest in the age group of 55–74. This is similar to the observation from population based data of developed countries. The age specific rates in older age group are much higher compared to that in pediatric, young and adult populations. This also demonstrates the limitation of hospital data to study burden of disease in a population as it suffers from problem of referal bias. Even though the age specific rates of CML in Mumbai are highest in age group of 55–74 years, they are still lower (less than half) compared to those observed by SEER registries.
However, the AAR observed by Mumbai registry for young and adult population are comparable, whereas higher in pediatric age group compared to those observed by SEER registries. This might be due to the fact that many cases of CML are asymptomatic or are accidentally diagnosed during routine health check-up. As routine health check-up is not common practice in India, many CML cases might not get registered, compared to developed countries like US where awareness and routine health check-up are common. It is unclear whether the higher incidence of CML in Mumbai in pediatric age group compared to SEER registries is real or due to misclassification of leukemia, which could be due to lack of diagnostic facilities in most of the centers. We also observed decrease in proportion of CML over the years compared to total leukemia, again possibly due to improvement in diagnosis of other leukemia types [Tables [Tables11 and and22].
We observed statistically significant decreasing trends in incidence of CML for both the gender during the recent 15-year period, but not for the whole 30-year period. It is unclear, whether this recent decreasing trend in incidence is because of the recent availability of genetic and molecular testing, which could reduce the misclassification of leukemia, and in particular can differentiate into myeloblastic syndrome and CML. However, it is possible that at least some percentage of myeloblostic syndromes could be classified as CML in absence of more recent diagnostic techniques. The decreasing trend in incidence of CML has been similarly observed by registries in the US, UK, and Denmark,[22–24] while in Poland the trends in incidence of CML were consistent during the period from 1960-1990.[25]
The natural history of CML has changed in recent years, partly due to earlier diagnosis but mostly as a consequence of the availability of effective therapies that have the potential to eradicate the Ph chromosome-positive clone.[26] There are many possible treatments for CML, but since 2001 the standard of care for newly diagnosed patients is imatinib therapy.[27] As more than 90% of patients taking this drug are in stable cytogenetic remission for atleast 5 years,[27,28] this has resulted in increase in survival from CML.[29] The imatinib therapy was started in some centers in Mumbai only in 2003. As the present data are only up to 2005, we have not observed any reduction in mortality from CML; however, the increase in survival due to effective therapy should result in decline in mortality in near future.
The availability of imatinib has changed the management of CML. Although the incidence rates of CML are low, its burden on population in terms of absolute numbers is quite high. Given the availability of reliable and simple diagnosis of CML, the public health goal should be to make sure the availability of proper diagnosis and management of CML across all the centers in urban and rural areas of developing world, so as to reduce the mortality. Currently, there have been limited studies to understand burden of CML in India and developing countries possibly because of current ICD classification scheme, where CML is classified on 4th digit and population-based registries usually produce the tables based on three digit ICD classification. It is important to observe the trends in incidence and mortality of CML over the years before celebrating success of recent diagnostic and management of CML.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared.