 PDF
PDF  Views
Views  Share
Share


CA-125 and risk of malignancy index for screening for malignancy in fertile aged females with ovarian cyst, which is more cost effectiveness?
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2013; 34(02): 72-73
DOI: DOI: 10.4103/0971-5851.116178
Abstract
Background: Ovarian tumor is a cause of infertility in the fertile-aged women. Also, it can also turns into malignancy and causes deadly outcome. Screening for malignancy is an important management. Aims: The available screening methods that are widely used at present include CA-125 determination and the risk of malignancy index (RMX), which is a combined CA-125 with ultrasonography, determination. Materials and Methods: Here, the author tries to assess cost-effectiveness of both alternative in screening by basic medical economics technique. Statistics: Classical descriptive analysis was used for cost effectiveness calculation. Results: In this work, from the cost-effectiveness analysis, the CA-125 test is more cost-effectiveness than RMX. Conclusion: This reflects that the usage of additional ultrasonography test for increasing the diagnostic activity in screening for ovarian cyst in the fertile aged females in Thailand is still not appropriate.
Publication History
Article published online:
20 July 2021
© 2013. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Background:
Ovarian tumor is a cause of infertility in the fertile-aged women. Also, it can also turns into malignancy and causes deadly outcome. Screening for malignancy is an important management.
Aims:
The available screening methods that are widely used at present include CA-125 determination and the risk of malignancy index (RMX), which is a combined CA-125 with ultrasonography, determination.
Materials and Methods:
Here, the author tries to assess cost-effectiveness of both alternative in screening by basic medical economics technique.
Statistics:
Classical descriptive analysis was used for cost effectiveness calculation.
Results:
In this work, from the cost-effectiveness analysis, the CA-125 test is more cost-effectiveness than RMX.
Conclusion:
This reflects that the usage of additional ultrasonography test for increasing the diagnostic activity in screening for ovarian cyst in the fertile aged females in Thailand is still not appropriate.
INTRODUCTION
Ovarian tumor is an important problem in female reproductive system and it can be the cause of infertility in the fertile-aged women.[1] Furthermore, it can also turns into malignancy and causes deadly outcome.[2,3,4] In ovarian tumor management, an important concept is to confirm that the existed ovarian tumor is not a malignancy mass.[2,3,4] Screening for this cancer is suggested in general gynecology practice. In general, the serum tumor marker, CA-125 is classically used as a screening tool. For the fertile-aged female, pre-menopause, the cut off value for CA-125 level is more than 200 U/ml. However, the sensitivity of the CA-125 is only about 70%.[5] Hence, there is a new modality for screening with the help of additional ultrasonography. The combined screening leads to the new parameters, risk of the malignancy index (RMX).[6] The RMX has a greater diagnostic sensitivity, up to 85.4%.[6] However, the cost of the test is increased. Here, the author tries to assess cost-effectiveness of both alternatives in screening by basic medical economics technique.
MATERIALS AND METHODS
This work is a medical economic study. The cost-effectiveness analysis is performed. The setting is Thailand. Cost in this work is mainly assigned as the price charge from the reference laboratory in Thailand (Special Laboratory, Bangkok) and present in baht (1 US dollar = 30 baht). The effectiveness in this work is assigned as the reported effectiveness in screening, the diagnostic sensitivity, and referred to the previous standard reference reports.[5,6,7] The cost-effectiveness analysis is carried out using the calculation for cost per effectiveness of each studied alternative (CA-125 and RMX).
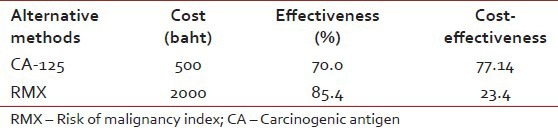
RESULTS
According to the cost-effectiveness analysis [Table 1], it seems that the cost per effectiveness of RMX is higher than that of CA-125.
Table 1
Cost-effectiveness analysis of alternative choices for screening for malignancy in ovarian tumor in fertile-aged women
DISCUSSION
Ovarian cyst is a big problem preventing full fertility in females. In addition to the basic obstacle to the reproduction, it can also take the possibility to turn into the malignant mass.[2,3,4] CA-125 is a widely used tumor marker that is indicated for screening for malignancy of ovarian cyst. Recently, a more modern alternative, RMX is presented. This method is CA-125 plus ultrasonography screening. The increased sensitivity is derived; however, it is still questionable for economical appropriateness. In this work, from the cost-effectiveness analysis, CA-125 is more cost effectiveness than RMX. This reflects that the usage of additional ultrasonography test for increasing the diagnostic activity in screening for ovarian cyst in fertile-aged women in Thailand is still not appropriate. This is also suggested for other similar settings with the same economic status.
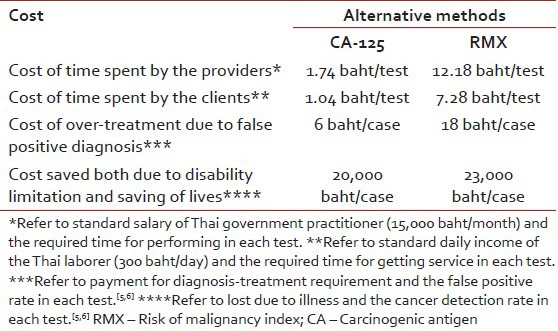
Nevertheless, the medico-economical consideration of the laboratory screening for ovarian mass must focus on the indirect costs.[8] Adding to the standard analysis based on cost of test, additional analysis on indirect costs, which include the cost of time spent by the providers, cost of time spent by the clients, cost of over-treatment due to false positive diagnosis and cost saved both due to disability limitation and saving of lives are also additionally assessed. Focusing on additional analysis on those indirect costs, the result is shown in Table 2. Of interest, the CA-125 still seems to be superior to RMX.
Table 2
Indirect costs of alternative choices for screening for malignancy in ovarian tumor in fertile-aged women
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.