 PDF
PDF  Views
Views  Share
Share


Bulky Pelvic Hodgkin Lymphoma in a Prepubertal Girl
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(02): 226-227
DOI: DOI: 10.4103/ijmpo.ijmpo_150_16
Abstract
Pure infra-diaphragmatic presentation is rare in pediatric Hodgkin lymphoma (HL). Isolated pelvic presentation is restricted to case reports in adults. We describe a unique presentation of HL as a primary pelvic disease in an 11-year-old prepubertal girl. She was treated based on the Euronet-Paediatric Hodgkin's Lymphoma Group protocol (EuroNet-PHL-C1) recommendations and assigned to treatment Group 2 (Stage IIB). The patient had bulky disease and a suboptimal response on interim 18-fluorodeoxyglucose positron emission tomography. The child was administered chemotherapy alone. Pelvic radiotherapy was consciously avoided due to the high risk of gonadal failure. She remains disease-free for 18 months now. Treatment of pediatric HL necessitates a delicate balance between achieving cure as well as avoiding serious late effects of therapy.
Keywords
Hypogonadism - infradiaphragmatic - late effects - positron emission tomography scan - radiationPublication History
Article published online:
06 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Pure infra-diaphragmatic presentation is rare in pediatric Hodgkin lymphoma (HL). Isolated pelvic presentation is restricted to case reports in adults. We describe a unique presentation of HL as a primary pelvic disease in an 11-year-old prepubertal girl. She was treated based on the Euronet-Paediatric Hodgkin's Lymphoma Group protocol (EuroNet-PHL-C1) recommendations and assigned to treatment Group 2 (Stage IIB). The patient had bulky disease and a suboptimal response on interim 18-fluorodeoxyglucose positron emission tomography. The child was administered chemotherapy alone. Pelvic radiotherapy was consciously avoided due to the high risk of gonadal failure. She remains disease-free for 18 months now. Treatment of pediatric HL necessitates a delicate balance between achieving cure as well as avoiding serious late effects of therapy.
Introduction
Primary sub-diaphragmatic pediatric Hodgkin lymphoma (HL) comprises merely 3% of all pediatric cases.[1] Isolated HL in the pelvis is rarely reported.[2,3] We report a prepubertal girl with a pelvic mass, which uniquely turned out to be HL. Besides chemotherapy, the management involved debating pros and cons of administering radiotherapy to the sensitive site.
Case Report
An 11-year-old girl presented with fever for 4 months. On examination, a left-sided suprapubic mass was palpated. Ultrasonography confirmed a mass in the pelvis. A magnetic resonance imaging revealed a large mass located in the pelvis, along with enlarged lymph nodes [Figure 1]. The initial clinical possibility was of a gonadal germ cell tumor. Serum alpha-fetoprotein and beta-human chorionic gonadotrophin were normal. A core biopsy was consistent with a diagnosis of HL, nodular sclerosis (NS) type. Immunohistochemistry was confirmatory; the large atypical cells were positive for CD15/CD30 and negative for CD20. An 18-fluorodeoxyglucose-positron emission tomography-computed tomography (FDG-PET-CT) confirmed FDG avidity of the mass and adjoining nodes. The bone marrow was not infiltrated.
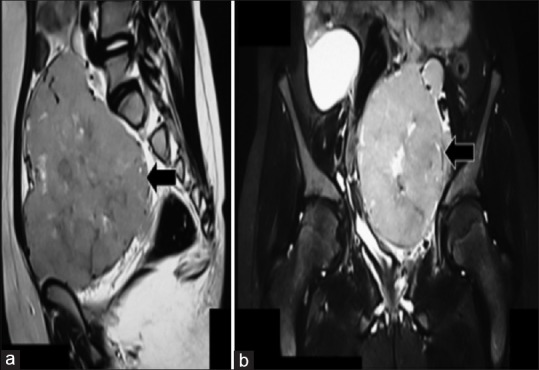
| Figure 1:Magnetic resonance imaging (a - sagittal view, b - coronal view) demonstrated a large pelvic mass (arrows in a and b). The left sided ovary was not distinctly identified. The uterus and urinary bladder were displaced and compressed by the mass
The patient was assigned to stage IIB and treatment - Group-2 of the Euronet-Paediatric Hodgkin's Lymphoma Group protocol (EuroNet-PHL-C1).[4] Two cycles of O-vincristine, E-etoposide, P-prednisone, A-adriamycin were administered. An interim FDG-PET-CT revealed >50% reduction of the mass, with a Deauville score (DS) of three, with complete resolution of the nodes. As per the guidelines of EuroNet-PHL-C1 trial, with a local partial remission and a DS of three, radiotherapy was indicated following two cycles of C-cyclophosphamide, O-vincristine, P-prednisone, DAC-dacarbazine (COPDAC). However, there was a major concern for infertility with radiotherapy to the pelvis. The multi-disciplinary team, along with the parents debated the options. The emerging international consensus was of DS of 1–3 being considered as a complete metabolic response at early interim PET.[5] Indeed, in the succeeding Euronet-C2 trial, the threshold of radiotherapy was to be raised to DS of 4–5, instead of 3–5.[6] The team opted to avoid radiotherapy and administer two additional (total: four) cycles of COPDAC, instead. An ultrasonography performed following six cycles of chemotherapy revealed a small cystic residual mass in the region of the left adenexa. A diagnostic laparoscopy performed to visualize and biopsy the mass demonstrated trivial bogginess of soft tissue in the pelvic wall with no visible mass. She has been well and in follow-up for 18 months.
Discussion
Primary infradiaphragmatic HL has been reported in 4%–13% of patients in studies encompassing all age groups.[7,8] Published literature on isolated pelvic disease is restricted to adults.[2,3] Infradiaphragmatic HL demonstrates distinct characteristics when compared to supradiaphragmatic disease such as older age, multiple involved sites, increased frequency of lymphocyte predominant histology, and a reduced frequency of NS variants.[7,8,9,10] Survival rates are not observed to be different, and recommendations for treatment do not differ.[4,7,8,9] Bulky disease with an inadequate response on interim FDG-PET is ideally radiated, albeit with increased risk of gonadal failure, premature menopause, and infertility in pelvic HL.[11] According to the Lugano classification for the management of lymphomas, DS-3 on interim FDG-PET indicates a favorable prognosis in most patients; interpretation must take into account timing of assessment, clinical context, and treatment.[5] We consciously avoided radiotherapy and administered two additional cycles of chemotherapy to avoid gonadal failure. A longer follow-up is necessary for ensuring a relapse-free period.
Conclusions
Pelvic HL is a rarity in children. The decision for radiotherapy is arduous due to the risk of infertility.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The inputs for management from Dr. Stephen Daw (Department Paediatric and Adolescent Oncology, University College London Hospital NHS Foundation Trust, London) and Dr. Rakesh Mittal (Ex-consultant, Kuwait Cancer Center, Ministry of Health, Kuwait) are gratefully acknowledged.
References
- Metzger M, Krasin MJ, Choi JK, Hudson MM. Hodgkin lymphoma. In: Pizzo PA, Poplack DG, editors. Principles and Practice of Pediatric Oncology. 7th ed. Philadelphia: Williams and Wilkins; 2015. p. 568-86.
- Kiran G, Canaz E, Sayar H, Serin S, Balakan O. Primary extranodal Hodgkin's lymphoma presenting with a single pelvic mass. J South Asian Fed Obstet Gynaecol 2014;6:183-6.
- Ha-Ou-Nou FZ, Benjilali L, Essaadouni L. Sacral pain as the initial symptom in primary Hodgkin's lymphoma of bone. J Cancer Res Ther 2013;9:511-3.
- Available from: https://www.skion.nl/workspace/uploads/EuroNet-PHL-Interim-Treatment-Guidelines-2012-12-3v0-2.pdf. [Last cited on 2016 Aug 06].
- Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J Clin Oncol 2014;32:3059-68.
- Second International Inter-Group Study for Classical Hodgkin Lymphoma in Children and Adolescents - Full Text View. Available from: https://www.clinicaltrials.gov/ct2/show/NCT02684708. [Last cited on 2016 Aug 07].
- Darabi K, Sieber M, Chaitowitz M, Braitman LE, Tester W, Diehl V. Infradiaphragmatic versus supradiaphragmatic Hodgkin lymphoma: A retrospective review of 1,114 patients. Leuk Lymphoma 2005;46:1715-20.
- Vassilakopoulos TP, Angelopoulou MK, Siakantaris MP, Konstantinou N, Symeonidis A, Karmiris T, et al. Pure infradiaphragmatic Hodgkin's lymphoma. Clinical features, prognostic factor and comparison with supradiaphragmatic disease. Haematologica 2006;91:32-9.
- Liao Z, Ha CS, Fuller LM, Hagemeister FB, Cabanillas F, Tucker SL, et al. Subdiaphragmatic stage I and II Hodgkin's disease: Long-term follow-up and prognostic factors. Int J Radiat Oncol Biol Phys 1998;41:1047-56.
- Cutuli B, Petit T, Hoffstetter S, Velten M, Dufour P, Giron C, et al. Treatment of subdiaphragmatic Hodgkin's disease: Long-term results and side effects. Oncol Rep 1998;5:1513-8.
- van Dorp W, van Beek RD, Laven JS, Pieters R, de Muinck Keizer-Schrama SM, van den Heuvel-Eibrink MM. Long-term endocrine side effects of childhood Hodgkin's lymphoma treatment: A review. Hum Reprod Update 2012;18:12-28.
| Figure 1:Magnetic resonance imaging (a - sagittal view, b - coronal view) demonstrated a large pelvic mass (arrows in a and b). The left sided ovary was not distinctly identified. The uterus and urinary bladder were displaced and compressed by the mass
References
- Metzger M, Krasin MJ, Choi JK, Hudson MM. Hodgkin lymphoma. In: Pizzo PA, Poplack DG, editors. Principles and Practice of Pediatric Oncology. 7th ed. Philadelphia: Williams and Wilkins; 2015. p. 568-86.
- Kiran G, Canaz E, Sayar H, Serin S, Balakan O. Primary extranodal Hodgkin's lymphoma presenting with a single pelvic mass. J South Asian Fed Obstet Gynaecol 2014;6:183-6.
- Ha-Ou-Nou FZ, Benjilali L, Essaadouni L. Sacral pain as the initial symptom in primary Hodgkin's lymphoma of bone. J Cancer Res Ther 2013;9:511-3.
- Available from: https://www.skion.nl/workspace/uploads/EuroNet-PHL-Interim-Treatment-Guidelines-2012-12-3v0-2.pdf. [Last cited on 2016 Aug 06].
- Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J Clin Oncol 2014;32:3059-68.
- Second International Inter-Group Study for Classical Hodgkin Lymphoma in Children and Adolescents - Full Text View. Available from: https://www.clinicaltrials.gov/ct2/show/NCT02684708. [Last cited on 2016 Aug 07].
- Darabi K, Sieber M, Chaitowitz M, Braitman LE, Tester W, Diehl V. Infradiaphragmatic versus supradiaphragmatic Hodgkin lymphoma: A retrospective review of 1,114 patients. Leuk Lymphoma 2005;46:1715-20.
- Vassilakopoulos TP, Angelopoulou MK, Siakantaris MP, Konstantinou N, Symeonidis A, Karmiris T, et al. Pure infradiaphragmatic Hodgkin's lymphoma. Clinical features, prognostic factor and comparison with supradiaphragmatic disease. Haematologica 2006;91:32-9.
- Liao Z, Ha CS, Fuller LM, Hagemeister FB, Cabanillas F, Tucker SL, et al. Subdiaphragmatic stage I and II Hodgkin's disease: Long-term follow-up and prognostic factors. Int J Radiat Oncol Biol Phys 1998;41:1047-56.
- Cutuli B, Petit T, Hoffstetter S, Velten M, Dufour P, Giron C, et al. Treatment of subdiaphragmatic Hodgkin's disease: Long-term results and side effects. Oncol Rep 1998;5:1513-8.
- van Dorp W, van Beek RD, Laven JS, Pieters R, de Muinck Keizer-Schrama SM, van den Heuvel-Eibrink MM. Long-term endocrine side effects of childhood Hodgkin's lymphoma treatment: A review. Hum Reprod Update 2012;18:12-28.