 PDF
PDF  Views
Views  Share
Share


Blueberry Muffin Baby: An Unusual Presentation of Infantile Neuroblastoma
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2018; 39(02): 263-265
DOI: DOI: 10.4103/ijmpo.ijmpo_183_17
Abstract
Neuroblastoma is the most common solid tumor of infancy presenting clinically in a plethora of different and sometimes unpredictable ways with a wide range of symptoms. Young children can present with bluish skin metastases that may resemble bruising secondary to child abuse. Blueberry muffin baby had been reported to be a manifestation of either dermal erythropoiesis secondary to some congenital viral infections or neoplastic infiltrations. Among the neoplastic diseases, neuroblastoma has been the most common association with these subcutaneous skin metastases. Here, we report 2 months infant with neuroblastoma who presented with abdominal distension and multiple blueberry muffin nodules.
Publication History
Article published online:
23 June 2021
© 2018. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Neuroblastoma is the most common solid tumor of infancy presenting clinically in a plethora of different and sometimes unpredictable ways with a wide range of symptoms. Young children can present with bluish skin metastases that may resemble bruising secondary to child abuse. Blueberry muffin baby had been reported to be a manifestation of either dermal erythropoiesis secondary to some congenital viral infections or neoplastic infiltrations. Among the neoplastic diseases, neuroblastoma has been the most common association with these subcutaneous skin metastases. Here, we report 2 months infant with neuroblastoma who presented with abdominal distension and multiple blueberry muffin nodules.
Introduction
Neuroblastoma is the most common extracranial solid tumor in childhood, accounting for more than 7% of malignancies in children younger than 15 years of age and 15% of all pediatric oncology deaths.[1] The most common presentation is as an abdominal mass, with 35% of cases arising from the adrenergic cells in the adrenal medulla. Other sites of origin are paraspinal ganglia (35%), posterior mediastinum (20%), and pelvis and neck (5%).[2] Distant metastatic disease at presentation is encountered in 60%–70% of children with the most commonly affected sites being the bone marrow, followed by the lymph nodes, liver, and skin.[3] Skin metastasis in the form of bluish, nontender subcutaneous nodules resembling blueberry muffins are seen almost exclusively in infants.[4]
Case Report
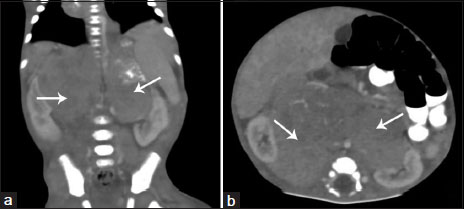
A 2-month-old male infant presented with 1 month history of multiple bluish skin nodules over trunk and extremities along with significant abdominal distension for 15 days. At admission, the child was lethargic, irritable, moderately pale, and undernourished. He had a pulse rate of 110/min, respiratory rate of 48/min, blood pressure of 84/52 mmHg, and SpO2 of 99% on room air. Multiple light bluish subcutaneous nodules [Figure 1] of 1–4 cm diameter were present all over the body. These mobile and nontender nodules were asymmetrically spread over trunk, extremities, and face. The abdomen was significantly distended and two large masses were palpable below the right and left costal margin. Rest of the systemic examination was unremarkable. Hematological evaluation revealed a hemoglobin of 7.7 g/dl, total leukocytes count of 6280/mm 3 (polymorph 22%, lymphocyte 66%), platelet count of 1.89 lakh/mm 3 and general blood picture suggestive of normocytic normochromic anemia. Ultrasonography abdomen revealed an enlarged liver with multiple hyperechoic well-defined rounded nodules. A large ill-defined heteroechoic lesion was seen in the right subhepatic region measuring 3.6 cm × 1.5 cm displacing the kidney anteromedially. Another similar lesion was seen in left lienorenal fossa measuring 3.9 cm × 2.8 cm displacing the left kidney. Contrast enhanced computed tomography (CECT) abdomen confirmed the presence of large heterogeneously enhancing bilateral paravertebral lesions merging in midline measuring approximately 7.7 cm × 7.3 cm × 6.4 cm [Figure 2]. Anteriorly, the lesion was causing displacement of pancreas, stomach, and bowel loops while laterally displacing bilateral kidneys with encasement of renal vessels. There was evidence of heterogeneous calcification within the lesion along with encasement of the aorta, celiac artery, superior mesenteric artery, and inferior vena cava. The liver was grossly enlarged with multiple heterogeneously enhancing nodular lesions of varying sizes in both lobes. Multiple heterogeneously enhancing calcified lesions were also seen in bilateral lung bases, superficial soft tissue of posterior abdominal wall, pelvic, and perineal soft tissues. Overall findings were suggestive of bilateral neuroblastoma with metastatic lesions involving liver, lungs, and superficial soft tissues. 24 h urinary vanillylmandelic acid (VMA) level was found to be elevated. A provisional diagnosis of bilateral neuroblastoma stage 4-S was made. For further confirmation and staging of the tumor, immunohistochemistry, exploratory laparotomy, and tumor biopsy were required. As our center was not having a specialized oncology department, we preferred to refer the child to a tertiary care oncology center for further management.

| Figure 1:Sagittal (a) and Coronal (b) sections of contrast enhanced computer tomography abdomen showing presence of large heterogeneously enhancing ill marginated lesions (arrows) in bilateral paravertebral location and merging in midline
| Figure.2:Blueberry muffin baby with multiple light bluish subcutaneous nodules over trunk and extremities
Discussion
Neuroblastoma is the most common solid tumor of infancy with a median age at presentation being 23 months.[2] Clinically, it may present with abdominal distension, proptosis, bone pain, pancytopenia, hypertension, watery diarrhea, and rarely subcutaneous skin nodules.[5] Young infants can present with bluish skin metastases in the form of subcutaneous nodules. These non-tender, bluish, and mobile nodules popularly known as “blueberry muffin sign” are almost exclusively seen in infants with stage 4-S neuroblastoma.[2],[4] Stage 4-S neuroblastoma is characterized by metastases confined to skin, liver, and bone marrow in infants younger than 1 year but no distant osseous metastasis.[6] Blueberry muffin baby is the morphologic term used to describe the appearance of nonblanching, bluish nodules in young babies. These eruptions are often generalized but favors the trunk, head, and neck. It had been reported to be a manifestation of either dermal erythropoiesis or neoplastic infiltrations. Among the neoplastic diseases with blueberry muffin babies, neuroblastoma is most commonly associated, whereas rhabdomyosarcoma, Langerhans cell histiocytosis, and leukemia are less frequently reported.[7] Abdominal ultrasonography is the preferred initial investigation if the abdominal mass is the presentation. CECT scan clearly delineate an abdominal mass with evidence of regional invasion, vascular encasement, lymphadenopathy, and calcification. Final diagnosis rests on pathological confirmation after examination of tumor tissue obtained by tru-cut biopsy in metastatic or nonresectable cases or during definitive surgery in localized resectable cases. Elevated urinary catecholamines support the diagnosis in over 90% of cases.[2] Patients with Stage IV-S disease have an excellent prognosis (>90%) without the use of adjuvant chemotherapy and radiotherapy.[8]
Conclusion
Neuroblastoma is one of the most common reported childhood malignancy, but sometimes, it can present in an extremely unpredictable manner. Infantile neuroblastoma, especially stage 4-S can present exclusively as multiple skin metastasis in the form of bluish subcutaneous nodules resembling blueberry muffins. Although blueberry muffin baby has conventionally been reported as a manifestation of dermal erythropoiesis in many congenital viral infections, the possibility of neoplastic infiltration and most commonly neuroblastoma should be taken into account. Although blueberry muffin as a presentation of stage 4-S neuroblastoma has been correlated well with excellent prognosis in most of the available literatures, its early detection will definitely help in timely management and overall prognosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
References
- Greengard E, Kayser CH, Bagatell R. Treatment of high-risk neuroblastoma in children: Recent clinic trial results. Clin Invest 2013; 3: 1071-81
- Hallett A, Traunecker H. A review and update on neuroblastoma. Paediatr Child Health 2012; 22: 103-7
- Papaioannou G, McHugh K. Neuroblastoma in childhood: Review and radiological findings. Cancer Imaging 2005; 5: 116-27
- Malis J. Clinical Presentation of Neuroblastoma. Available from: http://www.dx.doi.org/10.5772/55921. [Last accessed on 2017 Aug 20].
- Kalaskar RR, Kalaskar AR. Neuroblastoma in early childhood: A rare case report and review of literature. Contemp Clin Dent 2016; 7: 401-4
- Mondì V, Piersigilli F, Salvatori G, Auriti C. et al. The skin as an early expression of malignancies in the neonatal age: A review of the literature and a case series. Biomed Res Int 2015; 2015: 809406
- Hsiao YW, Tseng FW, Shih YL, Kuo TT, Jaing TH, Hui RC. Blueberry muffin baby with acute myeloid leukemia and spontaneous remission. Dermatol Sin 2011; 29: 47-9
- Chan AR, Johnston DH, Stoneman D. Disseminated neuroblastoma with initial presentation as an intraoral mass: Case report. Pediatr Dent 1994; 16: 310-3
Address for correspondence
Publication History
Article published online:
23 June 2021
© 2018. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2,
Noida-201301 UP, India
| Figure 1:Sagittal (a) and Coronal (b) sections of contrast enhanced computer tomography abdomen showing presence of large heterogeneously enhancing ill marginated lesions (arrows) in bilateral paravertebral location and merging in midline
| Figure.2:Blueberry muffin baby with multiple light bluish subcutaneous nodules over trunk and extremities
References
- Greengard E, Kayser CH, Bagatell R. Treatment of high-risk neuroblastoma in children: Recent clinic trial results. Clin Invest 2013; 3: 1071-81
- Hallett A, Traunecker H. A review and update on neuroblastoma. Paediatr Child Health 2012; 22: 103-7
- Papaioannou G, McHugh K. Neuroblastoma in childhood: Review and radiological findings. Cancer Imaging 2005; 5: 116-27
- Malis J. Clinical Presentation of Neuroblastoma. Available from: http://www.dx.doi.org/10.5772/55921. [Last accessed on 2017 Aug 20].
- Kalaskar RR, Kalaskar AR. Neuroblastoma in early childhood: A rare case report and review of literature. Contemp Clin Dent 2016; 7: 401-4
- Mondì V, Piersigilli F, Salvatori G, Auriti C. et al. The skin as an early expression of malignancies in the neonatal age: A review of the literature and a case series. Biomed Res Int 2015; 2015: 809406
- Hsiao YW, Tseng FW, Shih YL, Kuo TT, Jaing TH, Hui RC. Blueberry muffin baby with acute myeloid leukemia and spontaneous remission. Dermatol Sin 2011; 29: 47-9
- Chan AR, Johnston DH, Stoneman D. Disseminated neuroblastoma with initial presentation as an intraoral mass: Case report. Pediatr Dent 1994; 16: 310-3