 PDF
PDF  Views
Views  Share
Share


Assessment of Cancer Chemotherapy Needs in Patients Attending Tertiary Care Cancer Center, q: A Cross-Sectional Study
CC BY 4.0 · Indian J Med Paediatr Oncol 2025; 46(01): 049-056
DOI: 10.1055/s-0044-1787149
Abstract
Introduction Globally, 19.3 million new cancer cases were diagnosed in 2020, with over 10.0 million cancer deaths. Patients with cancer often face various long-term physical, social, financial, psychological, and existential challenges, complicating their survivorship.
Objectives This study aimed to evaluate the different needs of patients undergoing chemotherapy at a tertiary care cancer center.
Materials and Methods Data were collected from a tertiary care cancer center using purposive sampling. A total of 101 samples were collected over a 2-month period.
Results The majority of participants were female (61.4%), with 38.6%, being male. Most participants were in the third stage of cancer (57.4%), with 42.6%, in the fourth stage. Localized metastasis was observed in 83.2%, of participants. The most common symptoms were lack of appetite (59.4%) and nausea/vomiting (54.5%). Most participants rated the care provided by nurses during chemotherapy as good (86.1%). The majority had moderate needs (67.3%) during the treatment course.
Conclusion The study highlights significant needs in the physical and psychological domains among patients undergoing chemotherapy.
Keywords
cancer needs assessment - chemotherapy - physical needs - psychological needsPatient Consent
Informed consent was obtained from each participant before the commencement of the study.
Publication History
Article published online:
18 July 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
- A RESEARCH CRITIQUE ON THE LIVED-IN EXPERIENCES OF PATIENTS SUBJECTED TO CHEMOTHERAPY IN SELECTED HOSPITALS AT CHENNAIMalarvizhi M., Journal of Health and Allied Sciences NU, 2015
- Psychological Stress and Coping Resources during Primary Systemic Therapy for Breast Cancer. Results of a Prospective StudyVolker Tschuschke, Aktuelle Neurologie, 2017
- Psychological Stress and Coping Resources during Primary Systemic Therapy for Breast Cancer. Results of a Prospective StudyVolker Tschuschke, Geburtshilfe und Frauenheilkunde, 2017
- Depression in Cancer Patients: Magnitude of Problem and Factors ResponsibleKartick Rastogi, Indian Journal of Medical and Paediatric Oncology, 2019
- Drug utilization evaluation of anticancer drugs in a charitable hospitalManeesha Mathew, Indian Journal of Medical and Paediatric Oncology, 2019
- Attitudes to chemotherapy: comparing views of patients with cancer with those of doctors, nurses, and general public.M L Slevin, The BMJ, 1990
- Understanding provision of chemotherapy to patients with end stage cancer: qualitative interview study.Hilde M Buiting, The BMJ, 2011
- Why a pomegranate?P.G. Langley, The BMJ, 2000
- Cancer survivors report array of unmet needs many years after diagnosisZ. Kmietowicz, The BMJ, 2015
- Compliance, satisfaction, and quality of life of patients with colorectal cancer receiving home chemotherapy or outpatient treatment: a randomised controlled tr...Josep M. Borràs, The BMJ, 2001
Abstract
Introduction Globally, 19.3 million new cancer cases were diagnosed in 2020, with over 10.0 million cancer deaths. Patients with cancer often face various long-term physical, social, financial, psychological, and existential challenges, complicating their survivorship.
Objectives This study aimed to evaluate the different needs of patients undergoing chemotherapy at a tertiary care cancer center.
Materials and Methods Data were collected from a tertiary care cancer center using purposive sampling. A total of 101 samples were collected over a 2-month period.
Results The majority of participants were female (61.4%), with 38.6%, being male. Most participants were in the third stage of cancer (57.4%), with 42.6%, in the fourth stage. Localized metastasis was observed in 83.2%, of participants. The most common symptoms were lack of appetite (59.4%) and nausea/vomiting (54.5%). Most participants rated the care provided by nurses during chemotherapy as good (86.1%). The majority had moderate needs (67.3%) during the treatment course.
Conclusion The study highlights significant needs in the physical and psychological domains among patients undergoing chemotherapy.
Keywords
cancer needs assessment - chemotherapy - physical needs - psychological needsIntroduction
Cancer is a major disorder that causes millions of deaths worldwide. Cancer cells divide uncontrollably, leading to tumor growth and immune system dysfunction. Due to factors such as population ageing, tobacco use, radiation exposure, adopting a more sedentary lifestyle, and genetic predisposition, its incidence has increased in recent years.[1] Globally, 19.3 million new cancer cases have been diagnosed in 2020, with over 10.0 million cancer deaths.[2]
According to recently released cancer facts and figures reported by the International Agency for Research on Cancer, there has been an overall increase in the cancer burden in South Asia over the last decade. The region is now home to almost a quarter of new cancer cases globally and is also expected to have the highest growth rate among all other regions by 2030.[3] Cancer remains a largely dreaded illness and is usually associated with death, but this may not always be true. Although it is still one of the top three leading causes of death in India and several other developing countries, it can be managed if diagnosed early.[4]
The increase in cancer burden in India can be attributed to several factors, such as an ageing population, an unhealthy lifestyle, and an increase in obesity. While the proportion of people with cancers in older age groups is expected to increase, the proportion of people younger than 50 with cancer is also expected to increase. Certain risk factors for cancer, such as tobacco use, unhealthy diet, and alcohol consumption, are expected to increase, contributing to the country's increased cancer burden.[5]
As a result of the current advances in cancer treatment and the evolving landscape of clinical trials, more adults are surviving cancer and living longer than ever before. The most common cause of cancer death is lung cancer, with 1.8 million deaths predicted.[6]
Patients with cancer may experience varying degrees of long-term physical, social, financial, psychological, and existential distress, complicating their survivorship. Cancer survivors may experience physical and psychological symptoms beyond 10 years after treatment completion, even though some cancer-related concerns usually decrease over time. These symptoms may include fatigue, pain, and sleep difficulty.[7]
Despite providing chemotherapy, many patients experience various symptoms in the form of adverse effects, a major drawback of chemotherapy.[8] The physical domain describes the adverse effects of chemotherapy. Other unmet needs are also present during treatment, crucial for improving quality of life. Psychological factors also play a major role in quantifying the health-related quality of life in cancer patients who may experience different psychological disturbances during the treatment.[9]
In the context of increasing cancer burden and the significant impact of chemotherapy on patients' well-being and quality of life, it is essential to evaluate the specific needs of individuals undergoing this treatment. This study aimed to assess the needs of patients undergoing chemotherapy at a tertiary care cancer center. By understanding these needs, health care providers can address chemotherapy-related adverse effects and improve patient-centered care. The findings of this study will inform clinical practice, guide future research, and contribute to interventions that optimize the chemotherapy experience of patients. The main objectives of the study were to assess the needs of patients undergoing chemotherapy for cancer and determine factors associated with these needs.
Methodology
This study used a cross-sectional design to assess the different needs of cancer chemotherapy patients in a tertiary care cancer center. Data collection was conducted over 2 months using purposive sampling. The sample size of 101 participants was calculated based on a 2%. prevalence of cancer in the Mysuru district, Karnataka, India, with an absolute precision of 2.8%. and a confidence interval of 95%. Patients who provided informed consent and were free of psychological disorders were included. Those in terminal cancer stages were also included to capture a full range of experiences. Data was collected over 2 months through interviews using the validated Cancer Needs Assessment Tool-Chemotherapy (CNAT-CC) questionnaire.[10] The CNAT-CC has defined cutoff scores to classify needs as no need (0–25), moderate need (26–50), and high need (51–75).
The term “need” refers to cancer chemotherapy patients' perceived or identified requirements, demands, or necessities. These needs encompass various aspects such as physical symptoms, psychological well-being, information, support, and other elements essential for the comprehensive care and well-being of individuals receiving chemotherapy.
Data was entered in Microsoft Excel 2019 and analyzed using SPSS version 26 (licensed to the institution). Data analysis involved descriptive statistics in determining the frequency and percentage of different needs, and the chi-square test was used to explore the associations between dependent and independent variables. This study adhered to the ethical standards outlined in the 1964 Declaration of Helsinki and its later amendments. All procedures involving human participants were conducted following the guidelines of the Institutional Ethical Committee. The study was approved by the Institutional Ethical Committee (approval number: JSSMC/IEC/03072023). Informed consent was obtained from each participant before the commencement of the study.
Results
Data were collected from 101 participants. The majority of the participants in the current study were females (61.4%), and 38.6%, were men. Most participants in the current study belonged to the Hindu religion (92.1%), while 4%-belonged to Muslims and Christianity. From the current study participants, 54.5%-belonged to rural areas, whereas 45.5%, were from urban areas. Most participants in the current study were illiterate (33.7%), and 12.9%, had a diploma or degree.
Most of the participants in the current study were semiskilled (33.7%), and the least were unskilled (13.9%). The majority of the participants belonged to socioeconomic class II; that is, their income lies between 3,504 and 7,007 INR, and the least (5%) belonged to socioeconomic class V (1,050 INR and below). Most of the participants in the current study had joint families (49.5%), followed by nuclear families (42.6%) and three-generation families (7.9%).
Personal History and Disease Profiles
Most participants in the current study were in third stage of cancer (57.4%), and 42.6%, were in fourth stage. Localized metastasis was observed in 83.2%, (n = 84) of the participants. This indicates that cancer had metastasized locally from the original tumor to nearby lymph nodes or tissues for these patients but had not spread further to distant sites in the body. Regional tumors refer to cancer that has spread outside the original site to nearby organs, lymph nodes, or tissues. In this study, 4%, (n = 4) of participants had regional tumors, meaning their cancer had spread regionally from the primary site to adjacent organs or structures but not yet distantly throughout the body.
Comorbidities were absent in most participants (n = 85, 84.2%). Among those with comorbid conditions, diabetes was present in 3%, (n = 3), diabetes with cardiovascular disease in 3%, (n = 3), diabetes with hypertension in 5.9%, (n = 6), and hypertension alone in 4%, (n = 4). The majority of participants were undergoing chemotherapy (66.3%), followed by surgery + chemotherapy (14.9%), and triple therapy (surgery + chemotherapy + radiation) (12.9 %). Note that 33.7 had lung cancer and 17.8%, had rectal carcinoma, followed by breast carcinoma (12.9%), esophageal carcinoma (10.9%), and carcinoma of the stomach (8.9%). Acute leukemia was present in 5.9%, of the participants ([Table 1]).
|
Personal history |
||
|---|---|---|
|
n |
%. |
|
|
Stage of cancer |
||
|
3 |
58 |
57.4 |
|
4 |
43 |
42.6 |
|
Type of tumor |
||
|
Regional |
4 |
4.0 |
|
Localized metastasis |
84 |
83.2 |
|
Metastasis |
13 |
12.9 |
|
Comorbidities |
||
|
DM |
3 |
3.0 |
|
DM and CVD |
3 |
3.0 |
|
DM and HTN |
6 |
5.9 |
|
HTN |
4 |
4.0 |
|
Nil |
85 |
84.2 |
|
Treatment |
||
|
Chemotherapy |
67 |
66.3 |
|
Surgery + chemotherapy |
15 |
14.9 |
|
Chemotherapy and radiation |
6 |
5.9 |
|
Surgery + chemotherapy + radiation |
13 |
12.9 |
|
Type of Cancer |
||
|
Acute leukemia |
6 |
5.9 |
|
Carcinoma of breast |
13 |
12.9 |
|
Carcinoma of colon |
2 |
2.0 |
|
Carcinoma of esophagus |
11 |
10.9 |
|
Carcinoma of leiomyosarcoma |
3 |
3.0 |
|
Carcinoma of lung |
34 |
33.7 |
|
Carcinoma of ovary |
5 |
5.0 |
|
Carcinoma of rectum |
18 |
17.8 |
|
Carcinoma of stomach |
9 |
8.9 |
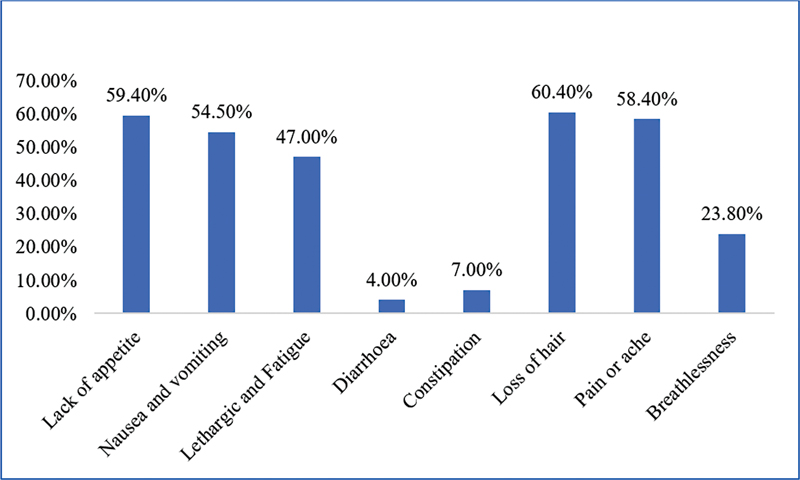
| Fig 1 Physical needs of the study participants.|
Psychological Domain
Regarding psychological symptoms, 33.7%, of the participants had anxiety and 9.9%, felt depressed. Some participants stated they felt stressed during chemotherapy (19.8%) and 11.9%, felt lonely.
Of the participants, 27.7%, said they feared chemotherapy sessions and 12.9%, said they feared hospitalization ([Table 2]).
|
Psychological domain |
Count N |
Column %. |
|
|---|---|---|---|
|
Feeling of anxiety |
No |
67 |
66.3 |
|
Yes |
34 |
33.7 |
|
|
Feeling of depressed |
No |
91 |
90.1 |
|
Yes |
10 |
9.9 |
|
|
Feeling stressed during treatment |
No |
81 |
80.2 |
|
Yes |
20 |
19.8 |
|
|
Feeling loneliness |
No |
89 |
88.1 |
|
Yes |
12 |
11.9 |
|
|
Fear of recurrence |
No |
92 |
91.1 |
|
Yes |
9 |
8.9 |
|
|
Fear of hospitalization |
No |
88 |
87.1 |
|
Yes |
13 |
12.9 |
|
|
Fear of chemotherapy sessions |
No |
74 |
73.3 |
|
Yes |
27 |
26.7 |
|
|
Fear of death |
No |
101 |
100.0 |
|
Yes |
0 |
0.0 |
|
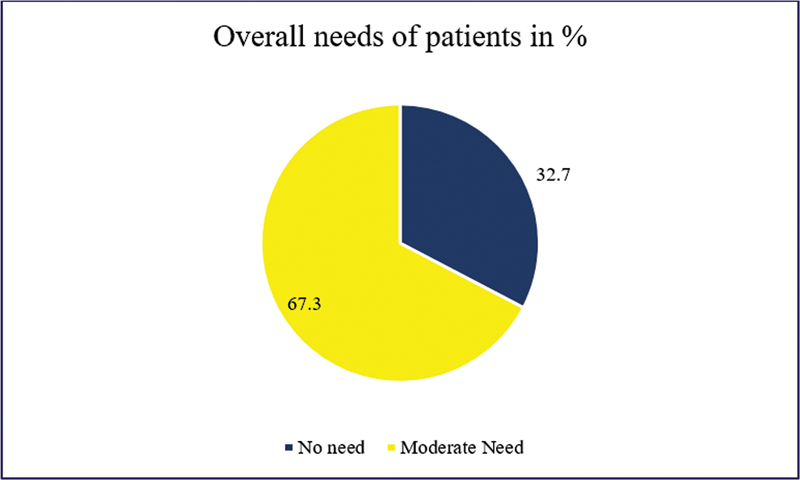
| Fig 2 Overall needs among the study participants.|
Factors Associated with Patient Needs
Sociodemographic factors associated with the participants' overall needs show that the family's socioeconomic status is associated with the overall needs with a chi-square value of 11.87 and a p-value of 0.01, which shows statistical significance.
Similarly, the type of family is associated with patients' overall needs with a chi-square value of 20.26 and a p-value of 0.001 that shows statistical significance ([Table 3]).
|
Sociodemographic variables |
Overall needs of patients |
||||||||
|---|---|---|---|---|---|---|---|---|---|
|
No need |
Moderate need |
High need |
|||||||
|
N |
%. |
N |
%. |
N |
%. |
Chi-square value |
p-Value |
||
|
Gender |
Male |
17 |
51.5 |
22 |
32.4 |
0 |
0.0 |
3.442 |
0.064[a] |
|
Female |
16 |
48.5 |
46 |
67.6 |
0 |
0.0 |
|||
|
Religion |
Hindu |
33 |
100.0 |
60 |
88.2 |
0 |
0.0 |
4.216 |
0.121[a] |
|
Christian |
0 |
0.0 |
4 |
5.9 |
0 |
0.0 |
|||
|
Muslim |
0 |
0.0 |
4 |
5.9 |
0 |
0.0 |
|||
|
Others |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
|||
|
Locality |
Urban |
11 |
33.3 |
35 |
51.5 |
0 |
0.0 |
2.947 |
0.086[a] |
|
Rural |
22 |
66.7 |
33 |
48.5 |
0 |
0.0 |
|||
|
Marital status |
Married |
33 |
100.0 |
68 |
100.0 |
0 |
0.0 |
4.005 |
0.549[a] |
|
unmarried |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
|||
|
Divorced |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
|||
|
Separated |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
|||
|
Widow/widower |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
|||
|
Education status of the head of the family |
Illiterate |
11 |
33.3 |
23 |
33.8 |
0 |
0.0 |
||
|
Primary education |
1 |
3.0 |
5 |
7.4 |
0 |
0.0 |
|||
|
Secondary education |
5 |
15.2 |
6 |
8.8 |
0 |
0.0 |
|||
|
High school education |
3 |
9.1 |
13 |
19.1 |
0 |
0.0 |
|||
|
Pre-university |
7 |
21.2 |
14 |
20.6 |
0 |
0.0 |
|||
|
Diploma/degree |
6 |
18.2 |
7 |
10.3 |
0 |
0.0 |
|||
|
Postgraduate |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
|||
|
Occupation status |
Unemployed |
12 |
36.4 |
12 |
17.6 |
0 |
0.0 |
4.710 |
0.194[a] |
|
Unskilled |
3 |
9.1 |
11 |
16.2 |
0 |
0.0 |
|||
|
Semiskilled |
9 |
27.3 |
25 |
36.8 |
0 |
0.0 |
|||
|
Skilled |
9 |
27.3 |
20 |
29.4 |
0 |
0.0 |
|||
|
Retired |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
|||
|
Living status |
Living alone |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
− |
− |
|
Living with spouse and children |
33 |
100.0 |
68 |
100.0 |
0 |
0.0 |
|||
|
Living with parents |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
|||
|
Others |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
|||
|
Socioeconomic status of the family |
7,008 and above |
6 |
18.2 |
1 |
1.5 |
0 |
0.0 |
11.878 |
0.018[b] |
|
3,504–3,503 |
20 |
60.6 |
46 |
67.6 |
0 |
0.0 |
|||
|
2,102–3,503 |
4 |
12.1 |
11 |
16.2 |
0 |
0.0 |
|||
|
1,051–2,101 |
3 |
9.1 |
5 |
7.4 |
0 |
0.0 |
|||
|
1,050 and below |
0 |
0.0 |
5 |
7.4 |
0 |
0.0 |
|||
|
Overall needs of patients |
|||||||||
|---|---|---|---|---|---|---|---|---|---|
|
No need |
Moderate need |
High need |
|||||||
|
Case history |
N |
%. |
N |
%. |
N |
%. |
Chi-square value |
p-Value |
|
|
Stage of cancer |
3 |
20 |
19.8 |
38 |
37.6 |
0 |
0.0 |
0.13 |
0.711 |
|
4 |
13 |
12.9 |
29 |
28.7 |
0 |
0.0 |
|||
|
Type of tumor |
Regional |
1 |
1.0 |
3 |
3.0 |
0 |
0.0 |
0.14 |
0.93 |
|
Localized metastasis |
28 |
27.7 |
56 |
55.4 |
0 |
0.0 |
|||
|
Metastasis |
4 |
4.0 |
9 |
8.9 |
0 |
0.0 |
|||
|
Unknown |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
|||
|
Comorbidities |
Diabetes mellitus |
0 |
0.0 |
3 |
3.0 |
0 |
0.0 |
9.34 |
0.043 |
|
Diabetes mellitus and cardiovascular disease |
0 |
0.0 |
3 |
3.0 |
0 |
0.0 |
|||
|
Diabetes mellitus and hypertension |
0 |
0.0 |
6 |
5.9 |
0 |
0.0 |
|||
|
Hypertension |
3 |
3.0 |
1 |
1.0 |
0 |
0.0 |
|||
|
Nil |
30 |
29.7 |
55 |
54.5 |
0 |
0.0 |
|||
|
Treatment |
Surgery |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
13.36 |
0.004[a] |
|
Chemotherapy |
22 |
21.8 |
45 |
44.6 |
0 |
0.0 |
|||
|
Radiation |
0 |
0.0 |
0 |
0.0 |
0 |
0.0 |
|||
|
Surgery + chemotherapy |
2 |
2.0 |
13 |
12.9 |
0 |
0.0 |
|||
|
Chemotherapy + radiation |
0 |
0.0 |
6 |
5.9 |
0 |
0.0 |
|||
|
Surgery + chemotherapy + radiation |
9 |
8.9 |
4 |
4.0 |
0 |
0.0 |
|||
|
Type of cancer |
Acute leukemia |
2 |
2.0 |
4 |
4.0 |
0 |
0.0 |
6.77 |
0.561 |
|
Breast cancer |
5 |
5.0 |
8 |
7.9 |
0 |
0.0 |
|||
|
Colon cancer |
0 |
0.0 |
2 |
2.0 |
0 |
0.0 |
|||
|
Esophageal cancer |
1 |
1.0 |
10 |
9.9 |
0 |
0.0 |
|||
|
Leiomyosarcoma |
1 |
1.0 |
2 |
2.0 |
0 |
0.0 |
|||
|
Lung cancer |
11 |
10.9 |
23 |
22.8 |
0 |
0.0 |
|||
|
Ovarian cancer |
1 |
1.0 |
4 |
4.0 |
0 |
0.0 |
|||
|
Rectal cancer |
9 |
8.9 |
9 |
8.9 |
0 |
0.0 |
|||
|
Stomach cancer |
3 |
3.0 |
6 |
5.9 |
0 |
0.0 |
|||
References
- What Is Cancer? - NCI. Accessed October 12, 2022 at: https://www.cancer.gov/about-cancer/understanding/what-is-cancer
- GLOBOCAN 2020 New Global Cancer Data | UICC. Accessed October 12, 2022 at: https://www.uicc.org/news/globocan-2020-new-global-cancer-data
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68 (06) 394-424
- Shah SC, Kayamba V, Peek Jr RM, Heimburger D. Cancer control in low- and middle-income countries: is it time to consider screening?. J Glob Oncol 2019; 5 (05) 1-8
- Anand P, Kunnumakkara AB, Sundaram C. et al. Cancer is a preventable disease that requires major lifestyle changes. Pharm Res 2008; 25 (09) 2097-2116
- Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- Wei D, Liu XY, Chen YY, Zhou X, Hu HP. Effectiveness of physical, psychological, social, and spiritual intervention in breast cancer survivors: an integrative review. Asia Pac J Oncol Nurs 2016; 3 (03) 226-232
- Homsi J, Walsh D, Rivera N. et al. Symptom evaluation in palliative medicine: patient report vs systematic assessment. Support Care Cancer 2006; 14 (05) 444-453
- Sitlinger A, Zafar SY. Health-related quality of life: the impact on morbidity and mortality. Surg Oncol Clin N Am 2018; 27 (04) 675-684
- Williamson S, Hack TF, Bangee M, Benedetto V, Beaver K. The patient needs assessment in cancer care: identifying barriers and facilitators to implementation in the UK and Canada. Support Care Cancer 2021; 29 (02) 805-12
- Chopra D, Rehan HS, Sharma V, Mishra R. Chemotherapy-induced adverse drug reactions in oncology patients: a prospective observational survey. Indian J Med Paediatr Oncol 2016; 37 (01) 42-46
- Chaturvedi SK. Psychiatric oncology: cancer in mind. Indian J Psychiatry 2012; 54 (02) 111-118
- Bhattacharyya S, Bhattacherjee S, Mandal T, Das DK. Depression in cancer patients undergoing chemotherapy in a tertiary care hospital of North Bengal, India. Indian J Public Health 2017; 61 (01) 14-18
- Komariah M, Rahayuwati L, Fitria N, Yulianita H, Lumbantobing VBM. Need Assessment on Patients with Advanced Stage Cancer. Eur J Mol Clin Med 2021; 8 (02) 974-85
- Meredith C, Symonds P, Webster L. et al. Information needs of cancer patients in west Scotland: cross sectional survey of patients' views. BMJ 1996; 313 (7059) 724-726
- Tariman JD, Doorenbos A, Schepp KG, Singhal S, Berry DL. Information needs priorities in patients diagnosed with cancer: a systematic review. J Adv Pract Oncol 2014; 2014 (05) 115-122
- Mekuria AB, Erku DA, Belachew SA. Preferred information sources and needs of cancer patients on disease symptoms and management: a cross-sectional study. Patient Prefer Adherence 2016; 10: 1991-1997
- Longo CJ, Fitch MI, Loree JM. et al. Patient and family financial burden associated with cancer treatment in Canada: a national study. Support Care Cancer 2021; 29 (06) 3377-3386
-
Mathew A,
George PS,
Ramadas K.
et al.
Sociodemographic factors and stage of cancer at diagnosis: a population-based study in South India. J Glob Oncol 2019; 5 (05) 1-10
Address for correspondence
Sunil Kumar D., MBBS, MD, PhDDepartment of Community Medicine, JSS Medical College, JSS Academy of Higher Education & Research (JSSAHER)SS Nagara, Mysuru, Karnataka 570015IndiaEmail: sunilkumard@jssuni.edu.inPublication History
Article published online:
18 July 2024© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, IndiaWe recommend- A RESEARCH CRITIQUE ON THE LIVED-IN EXPERIENCES OF PATIENTS SUBJECTED TO CHEMOTHERAPY IN SELECTED HOSPITALS AT CHENNAIMalarvizhi M., Journal of Health and Allied Sciences NU, 2015
- Psychological Stress and Coping Resources during Primary Systemic Therapy for Breast Cancer. Results of a Prospective StudyVolker Tschuschke, Aktuelle Neurologie, 2017
- Psychological Stress and Coping Resources during Primary Systemic Therapy for Breast Cancer. Results of a Prospective StudyVolker Tschuschke, Geburtshilfe und Frauenheilkunde, 2017
- Depression in Cancer Patients: Magnitude of Problem and Factors ResponsibleKartick Rastogi, Indian Journal of Medical and Paediatric Oncology, 2019
- Drug utilization evaluation of anticancer drugs in a charitable hospitalManeesha Mathew, Indian Journal of Medical and Paediatric Oncology, 2019
- Brief collaborative care intervention to reduce perceived unmet needs in highly distressed breast cancer patients: randomized controlled trialTatsuo Akechi, Japanese Journal of Clinical Oncology, 2020
- Psycho-Oncology: A Quick Reference on the Psychosocial Dimensions of Cancer Symptom ManagementJimmie C. Holland, Oxford Academic Books, 2014
- Association of a home-based nursing service during chemotherapy with the transfer to home care immediately after the last chemotherapy treatment in patients wit...Takahiro Higashibata, Japanese Journal of Clinical Oncology, 2022
- Psycho-Oncological Care and SurvivorshipLuzia Travado, Oxford Academic Books, 2019
- Cluster Analysis Demonstrates the Need to Individualize Care for Cancer Survivorsde Rooij, The Oncologist, 2018
- A RESEARCH CRITIQUE ON THE LIVED-IN EXPERIENCES OF PATIENTS SUBJECTED TO CHEMOTHERAPY IN SELECTED HOSPITALS AT CHENNAI
| | Fig 1 Physical needs of the study participants.|
| Fig 2 Overall needs among the study participants.|
References
- What Is Cancer? - NCI. Accessed October 12, 2022 at: https://www.cancer.gov/about-cancer/understanding/what-is-cancer
- GLOBOCAN 2020 New Global Cancer Data | UICC. Accessed October 12, 2022 at: https://www.uicc.org/news/globocan-2020-new-global-cancer-data
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68 (06) 394-424
- Shah SC, Kayamba V, Peek Jr RM, Heimburger D. Cancer control in low- and middle-income countries: is it time to consider screening?. J Glob Oncol 2019; 5 (05) 1-8
- Anand P, Kunnumakkara AB, Sundaram C. et al. Cancer is a preventable disease that requires major lifestyle changes. Pharm Res 2008; 25 (09) 2097-2116
- Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- Wei D, Liu XY, Chen YY, Zhou X, Hu HP. Effectiveness of physical, psychological, social, and spiritual intervention in breast cancer survivors: an integrative review. Asia Pac J Oncol Nurs 2016; 3 (03) 226-232
- Homsi J, Walsh D, Rivera N. et al. Symptom evaluation in palliative medicine: patient report vs systematic assessment. Support Care Cancer 2006; 14 (05) 444-453
- Sitlinger A, Zafar SY. Health-related quality of life: the impact on morbidity and mortality. Surg Oncol Clin N Am 2018; 27 (04) 675-684
- Williamson S, Hack TF, Bangee M, Benedetto V, Beaver K. The patient needs assessment in cancer care: identifying barriers and facilitators to implementation in the UK and Canada. Support Care Cancer 2021; 29 (02) 805-12
- Chopra D, Rehan HS, Sharma V, Mishra R. Chemotherapy-induced adverse drug reactions in oncology patients: a prospective observational survey. Indian J Med Paediatr Oncol 2016; 37 (01) 42-46
- Chaturvedi SK. Psychiatric oncology: cancer in mind. Indian J Psychiatry 2012; 54 (02) 111-118
- Bhattacharyya S, Bhattacherjee S, Mandal T, Das DK. Depression in cancer patients undergoing chemotherapy in a tertiary care hospital of North Bengal, India. Indian J Public Health 2017; 61 (01) 14-18
- Komariah M, Rahayuwati L, Fitria N, Yulianita H, Lumbantobing VBM. Need Assessment on Patients with Advanced Stage Cancer. Eur J Mol Clin Med 2021; 8 (02) 974-85
- Meredith C, Symonds P, Webster L. et al. Information needs of cancer patients in west Scotland: cross sectional survey of patients' views. BMJ 1996; 313 (7059) 724-726
- Tariman JD, Doorenbos A, Schepp KG, Singhal S, Berry DL. Information needs priorities in patients diagnosed with cancer: a systematic review. J Adv Pract Oncol 2014; 2014 (05) 115-122
- Mekuria AB, Erku DA, Belachew SA. Preferred information sources and needs of cancer patients on disease symptoms and management: a cross-sectional study. Patient Prefer Adherence 2016; 10: 1991-1997
- Longo CJ, Fitch MI, Loree JM. et al. Patient and family financial burden associated with cancer treatment in Canada: a national study. Support Care Cancer 2021; 29 (06) 3377-3386
- Mathew A, George PS, Ramadas K. et al. Sociodemographic factors and stage of cancer at diagnosis: a population-based study in South India. J Glob Oncol 2019; 5 (05) 1-10