 PDF
PDF  Views
Views  Share
Share


Androgen Receptor Expression in Triple Negative Breast Cancer - Study from a Tertiary Health Care Center in South India
CC BY-NC-ND 4.0 ? Indian J Med Paediatr Oncol 2018; 39(01): 28-31
DOI: DOI: 10.4103/ijmpo.ijmpo_4_17
Abstract
Background:?The treatment of breast cancer is based on a multi-modality approach. Analysis of the hormone receptor has been accepted as a standard procedure, in the routine management of breast cancer patients. Triple negative breast cancers (TNBCs) are those which are negative for expression of all three markers, i.e., estrogen receptor, progesterone receptor (PR), and human epidermal growth factor receptor. High expression of Ki-67, a proliferation index, has been associated with a worse prognosis in TNBC. TN cancers are aggressive in nature as they do not respond to routine targeted therapy. The role of the androgen receptor (AR) in breast carcinomas is important as AR has been suggested as a potential therapeutic target. We did this study to assess AR immunoreactivity in TNBCs and correlate with Ki-67 index.?Materials and Methods:?In this study group, there were 45 cases of TN invasive breast carcinomas. These tumors were analyzed with respect to AR and Ki-67 index.?Results:?Of 45 TN breast carcinomas analyzed, 42 were infiltrating duct cell carcinoma (IDCC) of not otherwise specified type. There were one medullary and two metaplastic carcinomas. The median age was 46 years. AR was positive in 20% (9/45) of cases. All the AR positive cases were an IDCC (nos). Out of the nine AR positive cases, six showed positivity for Ki-67. The statistical analysis using Pearson's Chi-squared method did not reveal any correlation between AR and Ki-67 index (P?= 0.574).?Conclusion:?Although our study did not reveal any statistically significant correlation between AR and Ki-67 index, assessment of AR status in TNBC patients is desirable as it may help to develop a targeted therapy in future in these aggressive cancers.
Keywords
Androgen receptor - breast cancer - Ki-67 index - triple negative breast cancer
Publication History
23 June 2021 (online)
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Background:?The treatment of breast cancer is based on a multi-modality approach. Analysis of the hormone receptor has been accepted as a standard procedure, in the routine management of breast cancer patients. Triple negative breast cancers (TNBCs) are those which are negative for expression of all three markers, i.e., estrogen receptor, progesterone receptor (PR), and human epidermal growth factor receptor. High expression of Ki-67, a proliferation index, has been associated with a worse prognosis in TNBC. TN cancers are aggressive in nature as they do not respond to routine targeted therapy. The role of the androgen receptor (AR) in breast carcinomas is important as AR has been suggested as a potential therapeutic target. We did this study to assess AR immunoreactivity in TNBCs and correlate with Ki-67 index.?Materials and Methods:?In this study group, there were 45 cases of TN invasive breast carcinomas. These tumors were analyzed with respect to AR and Ki-67 index.?Results:?Of 45 TN breast carcinomas analyzed, 42 were infiltrating duct cell carcinoma (IDCC) of not otherwise specified type. There were one medullary and two metaplastic carcinomas. The median age was 46 years. AR was positive in 20% (9/45) of cases. All the AR positive cases were an IDCC (nos). Out of the nine AR positive cases, six showed positivity for Ki-67. The statistical analysis using Pearson's Chi-squared method did not reveal any correlation between AR and Ki-67 index (P?= 0.574).?Conclusion:?Although our study did not reveal any statistically significant correlation between AR and Ki-67 index, assessment of AR status in TNBC patients is desirable as it may help to develop a targeted therapy in future in these aggressive cancers.
Keywords
Androgen receptor - breast cancer - Ki-67 index - triple negative breast cancer
Introduction
Breast cancer is one of the most common malignancies in females worldwide.[1] The incidence of breast carcinoma is rapidly increasing in India. Currently, according to the International Agency for Research on Cancer, breast cancer is the most common cancer in Indian females.[2] The treatment of breast cancer is based on a multi-modality approach.[1] Analysis of the hormone receptor has been accepted as a standard procedure, in the routine management of patients with breast cancer. Triple negative breast cancers (TNBCs) are those which are negative for expression of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor (HER-2 neu).[1],[3] TN is considered to be an aggressive form of breast cancer as they do not benefit from the standard targeted therapies.[1],[4] High expression of Ki-67, a proliferation index, has been associated with a worse prognosis in TNBC.[5]
The role of the androgen receptor (AR) in breast carcinomas has drawn great attention in recent years, especially due to its expression in ER and PR negative breast carcinomas.[1],[6] AR has been suggested as a potential therapeutic target.[1]
In this study, we have included consecutive TN cases for 1 year and attempted to correlate with AR receptor status and Ki 67 levels.
Materials and Methods
There were 148 cases of TN breast carcinomas (negative for ER, PR, and HER-2) in 10 year study. The criteria for determining triple negativity were based on immunohistochemical (IHC) staining. In TNBC patients, ER and PR staining were 0% by IHC, and HER2 staining was 0 by IHC or 1+.
In the present study, 45 consecutive cases of TN breast carcinomas, diagnosed in 1 year period, were retrospectively analyzed. In these 45 TN breast carcinoma cases, immunostaining for AR was done. This study was conducted in a single tertiary care institution from south India. We have excluded breast carcinoma cases from other health care centers, where paraffin blocks of were received only for review and IHC analysis due to unknown fixation status. In situ carcinomas and cases with incomplete information were also excluded from the study. The in-house specimens (modified radical mastectomy, lumpectomy, excisional biopsy, tru-cut) were fixed by 10% neutral buffered formalin were included in the study group. The histopathology and IHC reports (ER, PR, HER-2, and Ki-67) were accessed from the computerized hospital information system. AR immunostain was done on 3 ? paraffin sections on 3-amino propyl ethoxysilane coated slides. Antigen retrieval was done by pressure cooking for 5?10 min in Tris EDTA buffer, pH 9.0. IHC was done by Polymer HRP (Horse Radish Peroxidase) IHC detection system. Primary antibody used for AR staining was monoclonal mouse anti-human antibody (clone-F 39.4.1). Prostate carcinoma case was taken as positive control for AR. The clone used for Ki-67 was BGX-Ki67. The antibodies used were prediluted. All the markers were from BioGenex [Table 1].
|
Antigen |
Antibody |
Clone |
Manufacturer |
Dilution |
|---|---|---|---|---|
|
AR ? Androgen receptor |
||||
|
AR |
Monoclonal |
F 39.4.1 |
BioGenex |
Prediluted |
|
Ki-67 |
Monoclonal |
BGX-Ki-67 |
BioGenex |
Prediluted |
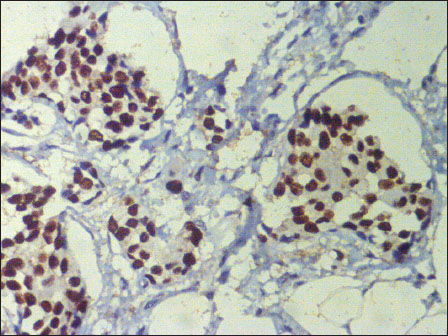
|?Figure.1Infiltrating duct cell carcinoma (nos) breast showing nuclear positivity for androgen receptor (immunohistochemistry, ?200)
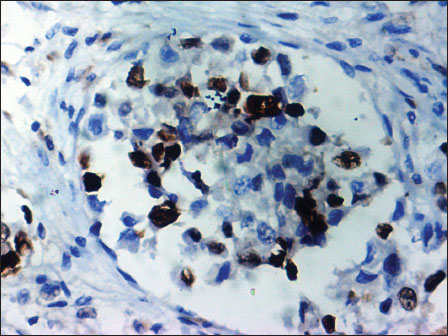
|?Figure.2Ki-67 nuclear positivity in infiltrating duct cell carcinoma (nos) breast (immunohistochemistry, ?400)
The data obtained was analyzed using the SPSS 11.5 (Chicago, IL, USA) statistical program. Pearson's Chi-squared method was used to obtain a correlation between AR and Ki-67.
Results
A total of 45 TN breast carcinomas were analyzed. There was one medullary and two metaplastic carcinomas among them, rest being infiltrating duct cell carcinoma (IDCC) not otherwise specified (IDC (nos)). The age range was wide (26?76 years). The median age was 46 years. AR was positive in 20% (9/45) cases. The AR positive cases were all IDCC (nos). Out of the nine AR positive cases, six showed high expression for Ki-67. The statistical analysis using Pearson's Chi-squared method did not reveal any correlation between AR and Ki-67 index (P?= 0.574).
Discussion
There is a sharp rise in breast cancer worldwide. Breast cancer is a leading cause of cancer death in the less developed countries of the world.[2] India also is witnessing an alarming rise of breast cancer.[7] ER and PR have gained widespread acceptance as independent prognostic parameters in breast carcinoma. Now a days, a standard work-up for breast carcinoma includes evaluation of ER, PR, and HER-2/neu status for therapeutic consideration. TN tumors are those which are negative for ER and PR as well as for HER2/neu. These tumors represent approximately 25% of all breast cancers.[1],[4]
In a previous study of breast carcinomas in 10 year study, we had observed 22.7% TN cases. However, there was no significant correlation between these TN cases and parameters such as age, tumor size, tumor grade, lymphadenopathy, and p53.[8]
The AR is expressed in normal breast tissue, its expression decreases as there is progression to in situ ductal carcinoma and invasive cancer.[9] AR is a member of the steroid hormone receptor family and is implicated in breast cancer pathogenesis. The current theory suggests that in breast carcinogenesis, the androgen signaling pathway plays a critical role independent of ER.[1],[4],[10] AR expression in normal luminal mammary epithelial cells is approximately 20%.[11] However, 70% of invasive and intraductal breast cancers express AR.[1],[4],[12],[13] A significant number of poorly differentiated breast carcinomas which are negative for ER and PR, are positive for AR.[11]
Recently, there is increasing interest regarding the role of the AR, particularly in patients with TN tumors. TN tumors generally have a more aggressive clinical course and do not benefit from conventional endocrine targeted therapies. However, recent evidence suggests that there may be role for AR as a therapeutic target for a subset of TNBC.[1],[4],[5],[6]
One study from India by Sharma?et al. noted 31.9% TNBC cases. They found that these cases present in younger females are associated with high grade, large tumor size, and high rate of lymph node positivity. The most common histological subtype in TNBC was IDC (nos).[3] In our study also most of the TN cases were IDC (nos). We found nine (20%) TN cases to be positive for AR. Most of the IHC studies have found the AR positive tumors represent a small subset within TNBCs, ranging from 12% to 23%.[14],[15] In a large study of over 2,000 invasive breast cancer, AR positivity was reported in 32% of TNBC.[14] Sutton?et al. observed that in 31.4% of TNBCs there is a positive expression of AR.[5] McGhan?et al., have described AR positive TN tumors to be more common in older patients, prone for lymph nodal metastasis and more advanced disease.[9] Whereas, Sutton?et al. noted that AR positive TNBCs are less likely to have distant metastasis.[5]
Bicalutamide is an oral, nonsteroidal, and AR antagonist.[14] A recently completed phase II trial of Bicalutamide in advanced TNBC involved a prospective screening step, in which TNBC tumors were assessed for AR expression before being assigned to therapy. The frequency of AR positivity by IHC was low (12%). This trial reported a clinical benefit rate of 19% and a median progression free survival of 12 weeks.[15]
Ki-67 is a proliferative marker with the highest expression during mitosis. Ki-67 is used as a prognostic marker in breast cancer. Higher expression of Ki-67 is associated with worse prognosis. In TNBCs, higher Ki-67 expression is associated with worse prognosis. Sutton?et al., observed a negative correlation between AR and Ki-67 expression. Hence, they opined that since AR positive tumors have lower Ki-67 index, high levels of AR may be associated with better prognosis in TN carcinomas. They have attributed this lower expression of Ki-67 in AR positive tumors, to the antiproliferative effect of AR.[5] However, we did not observe any statistically significant correlation between AR and Ki-67 expression in TNBCs, in our study.
Conclusion
In the current study, a subset of TNBCs (20%) are positive for AR. Antiandrogen therapy may be tried in those TNBCs expressing AR as the TN cancers do not respond to standard targeted therapy and are aggressive in nature. We did not find any significant correlation between AR and Ki-67 expression. However, results from multi-institutional studies with better sample size and follow-up data should be analyzed before advocating anti-androgen therapy for TNBCs showing AR positivity.
Conflict of Interest
There are no conflicts of interest.
Acknowledgments
The authors would like to thank Dr Aparna Bitla and senior technicians Mrs. Ushanandini and Mr. Ramana for their help.
References
- i JP, Yang YL, Zhu H, Wang J, Jia Y, Liu N.?et al.?Expression of the androgen receptor and its correlation with molecular subtypes in 980 Chinese breast cancer patients. Breast Cancer (Auckl) 2012; 6: 1-8
- erlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C.?et al. GLOBOCAN 2012 v 1.0, Cancer incidence and Mortality Worldwide: IARC Cancer Base No. 11. Lyon, France: International Agency for Research on Cancer; 2013. Available from: http://www.globocan,iarc.fr. [Last accessed on 2017 Oct 02]
- harma M, Sharma JD, Sarma A, Ahmed S, Kataki AC, Saxena R.?et al.?Triple negative breast cancer in people of North East India: Critical insights gained at a regional cancer centre. Asian Pac J Cancer Prev 2014; 15: 4507-11
- ahleh Z.?Androgen receptor as a target for the treatment of hormone receptor-negative breast cancer: An unchartered territory. Future Oncol 2008; 4: 15-21
- utton LM, Cao D, Sarode V, Molberg KH, Torgbe K, Haley B.?et al.?Decreased androgen receptor expression is associated with distant metastases in patients with androgen receptor-expressing triple-negative breast carcinoma. Am J Clin Pathol 2012; 138: 511-6
- hen J, Zhang X, Tian R, Liu Y, Dong HM, Guo RF.?et al.?Expression of androgen receptor in breast carcinoma and its relationship with estrogen receptor, progesterone receptor and HER2 status. Zhonghua Bing Li Xue Za Zhi 2010; 39: 743-6
- ational Cancer Registry Programme, Indian Council of Medical Research. Leading sites of cancer. In: Consolidated Report of Population Based Cancer Registries 2001-2004, Incidence and Distribution of Cancer. Bangalore: Coordinating Unit, National Cancer Registry Programme (ICMR); 2006.p.8-30
- atnayak R, Jena A, Rukmangadha N, Chowhan AK, Sambasivaiah K, Phaneendra BV.?et al.?Hormone receptor status (estrogen receptor, progesterone receptor), human epidermal growth factor-2 and p53 in South Indian breast cancer patients: A tertiary care center experience. Indian J Med Paediatr Oncol 2015; 36: 117-22
- cGhan LJ, McCullough AE, Protheroe CA, Dueck AC, Lee JJ, Sinha S.?et al.?Androgen receptor-positive triple negative breast cancer: A unique breast cancer subtype. Ann Surg Oncol 2014; 21: 361-7
- Lim E, Ni M, Cao S, Hazra A, Tamimi RM, Brown M.?et al.?Importance of breast cancer subtype in the development of androgen receptor directed therapy. Curr Breast Cancer Rep 2014; 6: 71-8
- Li S, Han B, Liu G, Li S, Ouellet J, Labrie F.?et al.?Immunocytochemical localization of sex steroid hormone receptors in normal human mammary gland. J Histochem Cytochem 2010; 58: 509-15
- Moinfar F, Okcu M, Tsybrovskyy O, Regitnig P, Lax SF, Weybora W.?et al.?Androgen receptors frequently are expressed in breast carcinomas: Potential relevance to new therapeutic strategies. Cancer 2003; 98: 703-11
- Gucalp A, Traina TA.?Triple-negative breast cancer: Role of the androgen receptor. Cancer J 2010; 16: 62-5
- Collins LC, Cole KS, Marotti JD, Hu R, Schnitt SJ, Tamimi RM.?et al.?Androgen receptor expression in breast cancer in relation to molecular phenotype: Results from the nurses' health study. Mod Pathol 2011; 24: 924-31
- Gucalp A, Tolaney S, Isakoff SJ, Ingle JN, Liu MC, Carey LA.?et al.?Phase II trial of bicalutamide in patients with androgen receptor-positive, estrogen receptor-negative metastatic breast cancer. Clin Cancer Res 2013; 19: 5505-12
Address for correspondence
Publication History
23 June 2021 (online)
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
|?Figure.1Infiltrating duct cell carcinoma (nos) breast showing nuclear positivity for androgen receptor (immunohistochemistry, ?200)
|?Figure.2Ki-67 nuclear positivity in infiltrating duct cell carcinoma (nos) breast (immunohistochemistry, ?400)
References
- i JP, Yang YL, Zhu H, Wang J, Jia Y, Liu N.?et al.?Expression of the androgen receptor and its correlation with molecular subtypes in 980 Chinese breast cancer patients. Breast Cancer (Auckl) 2012; 6: 1-8
- erlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C.?et al. GLOBOCAN 2012 v 1.0, Cancer incidence and Mortality Worldwide: IARC Cancer Base No. 11. Lyon, France: International Agency for Research on Cancer; 2013. Available from: http://www.globocan,iarc.fr. [Last accessed on 2017 Oct 02]
- harma M, Sharma JD, Sarma A, Ahmed S, Kataki AC, Saxena R.?et al.?Triple negative breast cancer in people of North East India: Critical insights gained at a regional cancer centre. Asian Pac J Cancer Prev 2014; 15: 4507-11
- ahleh Z.?Androgen receptor as a target for the treatment of hormone receptor-negative breast cancer: An unchartered territory. Future Oncol 2008; 4: 15-21
- utton LM, Cao D, Sarode V, Molberg KH, Torgbe K, Haley B.?et al.?Decreased androgen receptor expression is associated with distant metastases in patients with androgen receptor-expressing triple-negative breast carcinoma. Am J Clin Pathol 2012; 138: 511-6
- hen J, Zhang X, Tian R, Liu Y, Dong HM, Guo RF.?et al.?Expression of androgen receptor in breast carcinoma and its relationship with estrogen receptor, progesterone receptor and HER2 status. Zhonghua Bing Li Xue Za Zhi 2010; 39: 743-6
- ational Cancer Registry Programme, Indian Council of Medical Research. Leading sites of cancer. In: Consolidated Report of Population Based Cancer Registries 2001-2004, Incidence and Distribution of Cancer. Bangalore: Coordinating Unit, National Cancer Registry Programme (ICMR); 2006.p.8-30
- atnayak R, Jena A, Rukmangadha N, Chowhan AK, Sambasivaiah K, Phaneendra BV.?et al.?Hormone receptor status (estrogen receptor, progesterone receptor), human epidermal growth factor-2 and p53 in South Indian breast cancer patients: A tertiary care center experience. Indian J Med Paediatr Oncol 2015; 36: 117-22
- cGhan LJ, McCullough AE, Protheroe CA, Dueck AC, Lee JJ, Sinha S.?et al.?Androgen receptor-positive triple negative breast cancer: A unique breast cancer subtype. Ann Surg Oncol 2014; 21: 361-7
- Lim E, Ni M, Cao S, Hazra A, Tamimi RM, Brown M.?et al.?Importance of breast cancer subtype in the development of androgen receptor directed therapy. Curr Breast Cancer Rep 2014; 6: 71-8
- Li S, Han B, Liu G, Li S, Ouellet J, Labrie F.?et al.?Immunocytochemical localization of sex steroid hormone receptors in normal human mammary gland. J Histochem Cytochem 2010; 58: 509-15
- Moinfar F, Okcu M, Tsybrovskyy O, Regitnig P, Lax SF, Weybora W.?et al.?Androgen receptors frequently are expressed in breast carcinomas: Potential relevance to new therapeutic strategies. Cancer 2003; 98: 703-11
- Gucalp A, Traina TA.?Triple-negative breast cancer: Role of the androgen receptor. Cancer J 2010; 16: 62-5
- Collins LC, Cole KS, Marotti JD, Hu R, Schnitt SJ, Tamimi RM.?et al.?Androgen receptor expression in breast cancer in relation to molecular phenotype: Results from the nurses' health study. Mod Pathol 2011; 24: 924-31
- Gucalp A, Tolaney S, Isakoff SJ, Ingle JN, Liu MC, Carey LA.?et al.?Phase II trial of bicalutamide in patients with androgen receptor-positive, estrogen receptor-negative metastatic breast cancer. Clin Cancer Res 2013; 19: 5505-12