 PDF
PDF  Views
Views  Share
Share


An Unusual Site and Presentation of Sarcoma
CC BY-NC-ND 4.0 ? Indian J Med Paediatr Oncol 2020; 41(01): 66
DOI: DOI: 10.4103/ijmpo.ijmpo_52_20
 On immunohistochemistry (IHC), tumor cell was positive for desmin and myogenin and negative for CD45 and CD20. The final diagnosis of alveolar rhabdomyosarcoma (RMS)-lymphadenopathic form was given. It is the most common malignant soft-tissue tumor of childhood, but rare in adulthood, occurring in fewer than 5%. The lymphadenopathic form of alveolar RMS shows lymph node involvement as the first clinical manifestation in the absence of recognizable primary tumor. Differential diagnosis of small, round blue cell tumor should be considered and excluded by morphology and IHC.
On immunohistochemistry (IHC), tumor cell was positive for desmin and myogenin and negative for CD45 and CD20. The final diagnosis of alveolar rhabdomyosarcoma (RMS)-lymphadenopathic form was given. It is the most common malignant soft-tissue tumor of childhood, but rare in adulthood, occurring in fewer than 5%. The lymphadenopathic form of alveolar RMS shows lymph node involvement as the first clinical manifestation in the absence of recognizable primary tumor. Differential diagnosis of small, round blue cell tumor should be considered and excluded by morphology and IHC.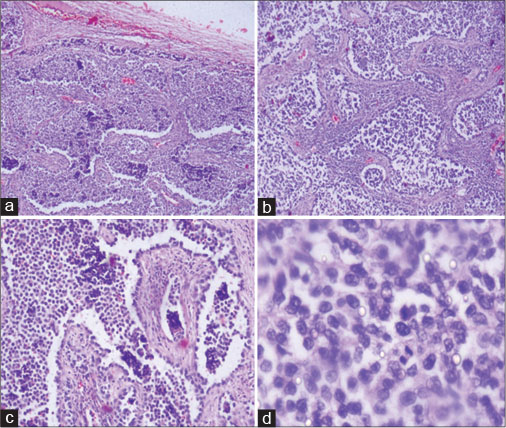
|?Fig. 1: (a?d) Neoplastic cells arranged in alveolar spaces separated by fibrous septae. The cells are small with scant cytoplasm and are adhering to the periphery of alveoli. Mitosis is brisk. (a = H and E, ?4; b = H and E, ?10; c = H and E, ?20; d = H and E, ?40)
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Publication History
Received: 10 February 2020
Accepted: 13 February 2020
Publication Date:
23 May 2021 (online)
? 2020. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
|?Fig. 1: (a?d) Neoplastic cells arranged in alveolar spaces separated by fibrous septae. The cells are small with scant cytoplasm and are adhering to the periphery of alveoli. Mitosis is brisk. (a = H and E, ?4; b = H and E, ?10; c = H and E, ?20; d = H and E, ?40)
On immunohistochemistry (IHC), tumor cell was positive for desmin and myogenin and negative for CD45 and CD20. The final diagnosis of alveolar rhabdomyosarcoma (RMS)-lymphadenopathic form was given. It is the most common malignant soft-tissue tumor of childhood, but rare in adulthood, occurring in fewer than 5%. The lymphadenopathic form of alveolar RMS shows lymph node involvement as the first clinical manifestation in the absence of recognizable primary tumor. Differential diagnosis of small, round blue cell tumor should be considered and excluded by morphology and IHC.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Address for correspondence
Publication History
Received: 10 February 2020
Accepted: 13 February 2020
Publication Date:
23 May 2021 (online)
? 2020. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
|?Fig. 1: (a?d) Neoplastic cells arranged in alveolar spaces separated by fibrous septae. The cells are small with scant cytoplasm and are adhering to the periphery of alveoli. Mitosis is brisk. (a = H and E, ?4; b = H and E, ?10; c = H and E, ?20; d = H and E, ?40)