 PDF
PDF  Views
Views  Share
Share


A Multicenter Retrospective Study to Evaluate Safety and Efficacy of Tocopheryl Polyethylene Glycol Succinate Docetaxel in Various Cancers
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2020; 41(04): 543-546
DOI: DOI: 10.4103/ijmpo.ijmpo_214_19
Abstract
Introduction
In order to overcome the polysorbate induced hypersensitivity reactions with chemotherapy drugs, novel drug-delivery mechanisms have been developed in the last decade. D-alpha-tocopheryl polyethylene glycol succinate (TPGS) is formed by esterification of alpha-tocopheryl succinate and polyethylene glycol 1000.
Materials and Methods
This was a real-world retrospective analysis designed to evaluate safety and efficacy of TPGS-docetaxel in various cancers. Patients hospitalized between June 2018 and May 2019 were included in the data set. While the efficacy was assessed by the Response Evaluation Criteria in Solid Tumors criteria, safety was assessed by the National Cancer Institute Common Terminology Criteria-adverse event (AE) criteria.
Results
A total of 61 patients who received at least one dose of TPGS-docetaxel were incorporated into the analysis set. The dose of TPGS docetaxel ranged from 20 mg/m2 to 120 mg/m2, commonly prescribed dose being 75 mg/m2. While 25 (40.98%) patients had a partial response, 17 (27.86%) patients had stable disease. Five (8.19%) patients progressed and 4 (6.55%) patients died during the chemotherapy, which was adjudicated to be unrelated to the drug as opined by the treating clinician. AE were reported in 42 patients in the safety data set. There were no AEs pertaining to hypersensitivity reported during the study. One AE of Grade 3 hand foot syndrome was encountered.
Conclusion
The preliminary evidence suggests that the novel TPGS-based docetaxel formulation is efficacious in various cancers, and importantly, it has an enhanced safety profile, as it is devoid of polysorbate 80 induced hypersensitivity reactions.
Keywords
Breast cancer - docetaxel - hypersensitivity reaction - non-small cell lung cancer - tocopheryl polyethylene glycol succinatePublication History
Received: 21 October 2019
Accepted: 01 June 2020
Article published online:
17 May 2021
© 2020. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Introduction
In order to overcome the polysorbate induced hypersensitivity reactions with chemotherapy drugs, novel drug-delivery mechanisms have been developed in the last decade. D-alpha-tocopheryl polyethylene glycol succinate (TPGS) is formed by esterification of alpha-tocopheryl succinate and polyethylene glycol 1000.
Materials and Methods
This was a real-world retrospective analysis designed to evaluate safety and efficacy of TPGS-docetaxel in various cancers. Patients hospitalized between June 2018 and May 2019 were included in the data set. While the efficacy was assessed by the Response Evaluation Criteria in Solid Tumors criteria, safety was assessed by the National Cancer Institute Common Terminology Criteria-adverse event (AE) criteria.
Results
A total of 61 patients who received at least one dose of TPGS-docetaxel were incorporated into the analysis set. The dose of TPGS docetaxel ranged from 20 mg/m2 to 120 mg/m2, commonly prescribed dose being 75 mg/m2. While 25 (40.98%) patients had a partial response, 17 (27.86%) patients had stable disease. Five (8.19%) patients progressed and 4 (6.55%) patients died during the chemotherapy, which was adjudicated to be unrelated to the drug as opined by the treating clinician. AE were reported in 42 patients in the safety data set. There were no AEs pertaining to hypersensitivity reported during the study. One AE of Grade 3 hand foot syndrome was encountered.
Conclusion
The preliminary evidence suggests that the novel TPGS-based docetaxel formulation is efficacious in various cancers, and importantly, it has an enhanced safety profile, as it is devoid of polysorbate 80 induced hypersensitivity reactions.
Keywords
Breast cancer - docetaxel - hypersensitivity reaction - non-small cell lung cancer - tocopheryl polyethylene glycol succinateIntroduction
Docetaxel is a second-generation taxane, derived from the inactive 10-deacetylbaccatin III, extracted from the European Yew tree (Taxus baccata).[1] In the formulation of the innovator docetaxel, polysorbate 80 (Tween 80) is used as a solubilizer, stabilizer and as an emulsifier. The administration of docetaxel polysorbate 80 formulation is through intravenous route by further diluting it in ethanol/water.[2]
A meticulous review of literature suggests that polysorbate 80 is responsible for causing hypersensitivity reactions when used as a solubilizer, not only with docetaxel but also with other chemotherapy agents.[3],[4] Despite the premedications, 10%–20% of the taxane pretreated patients experience hypersensitivity reaction with docetaxel.[5] Based on the mortality data, the United States Food and Drug Administration (US FDA) has issued a “black box” warning on the package insert.[6] In order to overcome these adverse reactions, D-alpha-tocopheryl polyethylene glycol succinate (TPGS), a novel drug-delivery mechanism, formed by esterification of alpha-tocopheryl succinate and polyethylene glycol (PEG) 1000, has been developed.[7] TPGS is a US FDA approved pharmaceutical adjuvant, a derivative of Vitamin E, which is water soluble and chemically comprises of a hydrophilic head portion and lipophilic alkyl tail.[8],[9] TPGS acts as an absorption enhancer, emulsifier, solubilizer, permeation enhancer and a stabilizer.[7],[9] Importantly, when co-administered with a chemotherapy agent, TPGS has shown to enhance drug solubility and inhibit P-glycoprotein mediated multidrug resistance.[10] In addition, properties of TPGS includes anti-cancer activity and anti-allergic actions mediated through decreasing immunoglobulin E (IgE), leukotrienes and histamines. Hence, prudently, it has been formulated with chemotherapy agents such as paclitaxel, 5-fluro uracil, cisplatin and mitoxantrone.[7],[11],[12] [Figure 1] summarizes some properties of TPGS-docetaxel.
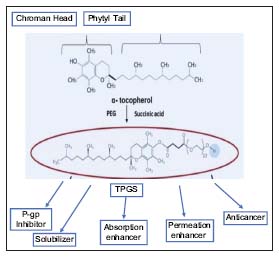
| Figure 1:Properties of tocopheryl polyethylene glycol succinate-docetaxel[9]
In the context of docetaxel, given that docetaxel by itself can cause hypersensitivity reactions,[13],[14],[15] TGPS-based micelle drug delivery system may be advantageous, as it can encapsulate hydrophobic docetaxel and thereby prevent the exposure to nondesirable sites, leading to decreased hypersensitive reaction. Taking into account, first, that more drug is delivered at the site of action,[7] and second, the anti-cancer and antidrug-resistant properties of TPGS,[10],[16] the new formulation may offer several advantages. Considering these factors and data from pharmacokinetic and pharmacodynamic study (unpublished data), the drug controller general of India has approved this formulation in 2013 without a Phase III study, as the active ingredient, docetaxel, was an established molecule with well-documented adverse events (AEs). However, in spite of this, it is important to know the efficacy and safety of the new formulation in real-world clinical settings and manage expectation postapproval. Therefore, we decided to observe the real-world usage, prescribing pattern and outcomes of docetaxel TPGS, a novel formulation without polysorbate 80.
Materials and Methods
This was a real-world retrospective analysis designed to evaluate safety and efficacy of TPGS-docetaxel in various cancers. Patients hospitalized between June 2018 and May 2019 were included in the data set. Hospital medical records (electronic or physical), outpatient department registers and laboratory record values were used to extract the data. As this was a real-world experience study, we used broad inclusion criteria to get a precise clinical picture of the patients who were administered the novel TPGS-docetaxel preparation. Physicians had prescribed the medication according to their preference based on clinical evidence and local hospital protocols. Patients of either sex, patients above 18 years of age, and all patients given TPGS-docetaxel for any of the following indications - (a) patients with locally advanced or metastatic breast cancer, (b) patients with hormone-refractory metastatic prostate cancer, (c) patients with locally advanced squamous cell carcinoma of the head and neck, (d) patients with advanced gastric adenocarcinoma, and (e) any other cancer which the investigator felt that TPGS docetaxel is useful, were included in the final analysis set.
Data were collected for knowing the patients baseline characteristics, comorbidities, dosage of docetaxel that was administered, efficacy and safety parameters. Further, to evaluate efficacy, the Response Evaluation Criteria in Solid Tumors 1.1 was used.[17] The results were presented in terms of frequency percentage of patients for complete response, partial response, stable disease, and progressive disease categories. Severities of the AEs are graded from 1 to 5 according to the US National Cancer Institute Common Terminology Criteria-AE criteria version 3.0.[18] The AEs were summarized as frequencies and percentages by type of reactions. Furthermore, in order to present the overall findings, descriptive statistics-percentages, frequency was used as appropriate.
Results
Patient demographics
A total of 61 patients who received at least one dose of TPGS-docetaxel were incorporated into the analysis set. [Table 1] demonstrates the characteristics of the study population at baseline. The majority of the patients (43 [70.4%]) were females and the average age of the patients was 48.8 years. In the analyzed cohort, 38 patients had a diagnosis of breast cancer (62.29%) 10 patients had head and neck squamous cell carcinoma (6.1%), 5 patients had gastric cancer (8.19%), 3 patients had hormone-resistant prostate cancer (4.91%), and one patient each with carcinoma esophagus (1.63%), carcinoma cervix (1.63%), leiomyosarcoma (1.63%), adenocarcinoma of unknown primary, and 1 (1.63%) carcinoma gall bladder (1.63%).
|
n (%) |
|
|---|---|
|
HNSCC – Head and neck squamous cell carcinoma; HRPC – Hormone resistant prostate cancer |
|
|
Total number of patients |
61 |
|
Sex distribution |
|
|
Male |
18 (29.5) |
|
Females |
43 (70.4) |
|
Diagnosis |
|
|
Breast cancer |
38 (62.29) |
|
HNSCC |
10 (6.1) |
|
Gastric cancer |
5 (8.9) |
|
HRPC |
3 (4.91) |
|
Carcinoma esophagus |
1 (1.63) |
|
Carcinoma cervix |
1 (1.63) |
|
Leiomyosarcoma |
1 (1.63) |
|
Metastatic adenocarcinoma |
1 (1.63) |
|
Carcinoma gall bladder |
1 (1.63) |
|
n (%) |
|
|---|---|
|
Partial response |
25 (40.98) |
|
Stable disease |
17 (27.86) |
|
Progressive disease |
5 (8.19) |
|
Death |
4 (6.55) |
|
Not evaluable |
2 (3.27) |
|
Total AE, n (%) |
AE of Grade 3 or more, n (%) |
|
|---|---|---|
|
AE – Adverse event |
||
|
Fatigue |
20 (47.6) |
0 |
|
Neurosensory symptoms |
10 (23.8) |
0 |
|
Pedal edema |
5 (11.9) |
0 |
|
Neutropenia |
3 (7.1) |
0 |
|
Hand foot syndrome |
2 (4.7) |
1 |
|
Pleural effusion |
1 (2.3) |
0 |
|
Mucositis |
1 (2.3) |
0 |
|
Hypersensitivity/anaphylaxis |
0 |
0 |
| Figure 1:Properties of tocopheryl polyethylene glycol succinate-docetaxel[9]
References
- Cortes JE, Pazdur R. Docetaxel. J Clin Oncol 1995; 13: 2643-55
- Engels FK, Mathot RA, Verweij J. Alternative drug formulations of docetaxel: A review. Anticancer Drugs 2007; 18: 95-103
- Picard M, Castells MC. Re-visiting hypersensitivity reactions to taxanes: A comprehensive review. Clin Rev Allergy Immunol 2015; 49: 177-91
- ed">4 Schwartzberg LS, Navari RM. Safety of polysorbate 80 in the oncology setting. Adv Ther 2018; 35: 754-67
- Vasey PA, Atkinson R, Coleman R, Crqaford M, Cruikshank M, Eggleton P. et al. Docetaxel-carboplatin as first line chemotherapy for epithelial ovarian cancer. Br J Cancer 2001; 84: 170-8
- Docetaxel Prescribing Information. United States Food and Drug Administration. 2014 https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/202356s000lbl.pdf Available from: [Last accessed on 2020 Jan 16]
- Neophytou CM, Constantinou AI. Drug delivery innovations for enhancing the anticancer potential of Vitamin E isoforms and their derivatives. Biomed Res Int 2015; 2015: 584862
- Zhang Z, Tan S, Feng SS. Vitamin E TPGS as a molecular biomaterial for drug delivery. Biomaterials 2012; 33: 4889-906
- Guo Y, Luo J, Tan S, Otieno BO, Zhang Z. The applications of Vitamin E TPGS in drug delivery. Eur J Pharm Sci 2013; 49: 175-86
- Dintaman JM, Silverman JA. Inhibition of P-glycoprotein by D-alpha-tocopheryl polyethylene glycol 1000 succinate (TPGS). Pharm Res 1999; 16: 1550-6
- Muthu MS, Kulkarni SA, Raju A, Feng SS. Theranostic liposomes of TPGS coating for targeted co-delivery of docetaxel and quantum dots. Biomaterials 2012; 33: 3494-501
- Zhu H, Chen H, Zeng X, Wang Z, Zhang X, Wu Y. et al. Co-delivery of chemotherapeutic drugs with Vitamin E TPGS by porous PLGA nanoparticles for enhanced chemotherapy against multi-drug resistance. Biomaterials 2014; 35: 2391-400
- Mertens WC, Eisenhauer EA, Jolivet J, Ernst S, Moore M, Muldal A. Docetaxel in advanced renal carcinoma. A phase II trial of the National Cancer Institute of Canada Clinical Trials Group. Ann Oncol 1994; 5: 185-7
- Pazdur R, Lassere Y, Soh LT, Ajani JA, Bready B, Soo E. et al. Phase II trial of docetaxel (Taxotere) in metastatic colorectal carcinoma. Ann Oncol 1994; 5: 468-70
- Weiss RB, Donehower RC, Wiernik PH, Ohnuma T, Gralla RJ, Trump DL. et al. B. Hypersensitivity reactions from taxol. J Clin Oncol 1990; 8: 1263-8
- Youk HJ, Lee E, Choi MK, Lee YJ, Chung JH, Kim SH. et al. Enhanced anticancer efficacy of alpha-tocopheryl succinate by conjugation with polyethylene glycol. J Control Release 2005; 107: 43-52
- Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R. et al. New response evaluation criteria in solid tumours: Revised RECIST Guideline (version 1.1). Eur J Cancer 2009; 45: 228-47
- Trotti A, Colevas AD, Setser A, Rusch V, Jaques D, Budach V. et al. CTCAE v3.0: Development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol 2003; 13: 176-81
- Suvarna VR. Real world evidence (RWE) – Are we (RWE) ready?. Perspect Clin Res 2018; 9: 61-3
- Figgitt DP, Wiseman LR. Docetaxel: An update of its use in advanced breast cancer. Drugs 2000; 59: 621-51
- Sjöström J, Blomqvist C, Mouridsen H, Pluzanska A, Ottosson-Lönn S, Bengtsson NO. et al. Docetaxel compared with sequential methotrexate and 5-fluorouracil in patients with advanced breast cancer after anthracycline failure: A randomised phase III study with crossover on progression by the Scandinavian Breast Group. Eur J Cancer 1999; 35: 1194-201
- Schellekens H, Hennink WE, Brinks V. The immunogenicity of polyethylene glycol: Facts and fiction. Pharm Res 2013; 30: 1729-34
- Shahar E, Hassoun G, Pollack S. Effect of Vitamin E supplementation on the regular treatment of seasonal allergic rhinitis. Ann Allergy Asthma Immunol 2004; 92: 654-8
- Yamada K, Hung P, Yoshimura K, Taniguchi S, Lim BO, Sugano M. Effect of unsaturated fatty acids and antioxidants on immunoglobulin production by mesenteric lymph node lymphocytes of Sprague-Dawley rats. J Biochem Tokyo 1996; 120: 138-44